Arterial revascularization, either endovascular and/or surgical, is the standard procedure for the treatment of patients with lower limb ischemia [1].
In Europe, it is estimated that 40 million individuals are affected by peripheral artery disease (PAD), with a prevalence of approximately 5.3%, based on a population of 750 million inhabitants [2].
Despite the availability of numerous endovascular and surgical techniques for treating lower limb ischemia, a subset of patients is not eligible for revascularization procedures and is therefore classified as “no-option”.
In the absence of restored blood flow, chronic limb-threatening ischemia (CLTI) in no-option patients characterized by pain, non-healing wounds, and gangrene typically progresses to major amputation (above the ankle).
Major amputation due to CLTI is associated with a 50% one-year mortality rate in patients over 65 years old, with even higher mortality among those with concomitant cardiovascular diseases [3].
Transcatheter arterialization of deep veins is an endovascular revascularization technique used to treat no-option chronic limb-threatening ischemia.
When performed in the lower limbs, the procedure involves creating an arteriovenous fistula proximal to the diseased tibial arteries using a covered stent. Oxygenated blood is thus diverted from the tibial arteries into the tibial veins, bypassing the severely diseased arterial segment. The venous system is then utilized to deliver oxygenated arterial blood to the foot through the plantar veins, potentially avoiding major amputation and promoting wound healing [4].
Patients considered for the procedure must be carefully selected, as it is contraindicated under specific conditions. These include the absence of an adequate patent deep or superficial venous axis, which requires a target vein that is sufficiently patent and free of thrombosis. Recent or extensive deep vein thrombosis (DVT) precludes the use of veins for retrograde arterial perfusion. Uncontrolled systemic infection or sepsis significantly increases perioperative risk. Advanced, uncompensated heart failure (e.g., NYHA class IV) cannot tolerate the increased afterload caused by the arteriovenous shunt. Severe coagulopathy or active bleeding poses a high risk of hemorrhagic complications. Lastly, advanced malignancy with limited life expectancy renders the procedure futile.
In this paper, we reported a case of a geriatric patient with diabetic foot and a high risk of major limb amputation based on clinical presentation.
According to the WIfI classification (3-3-2), the patient’s overall stage of 4 corresponded to an estimated 1-year amputation risk of 20–50% [5].
Considering the high 5-year mortality rate associated with major amputation in elderly diabetic patients, lower limb arterialization proved to be a valuable option for preventing limb loss in this case.
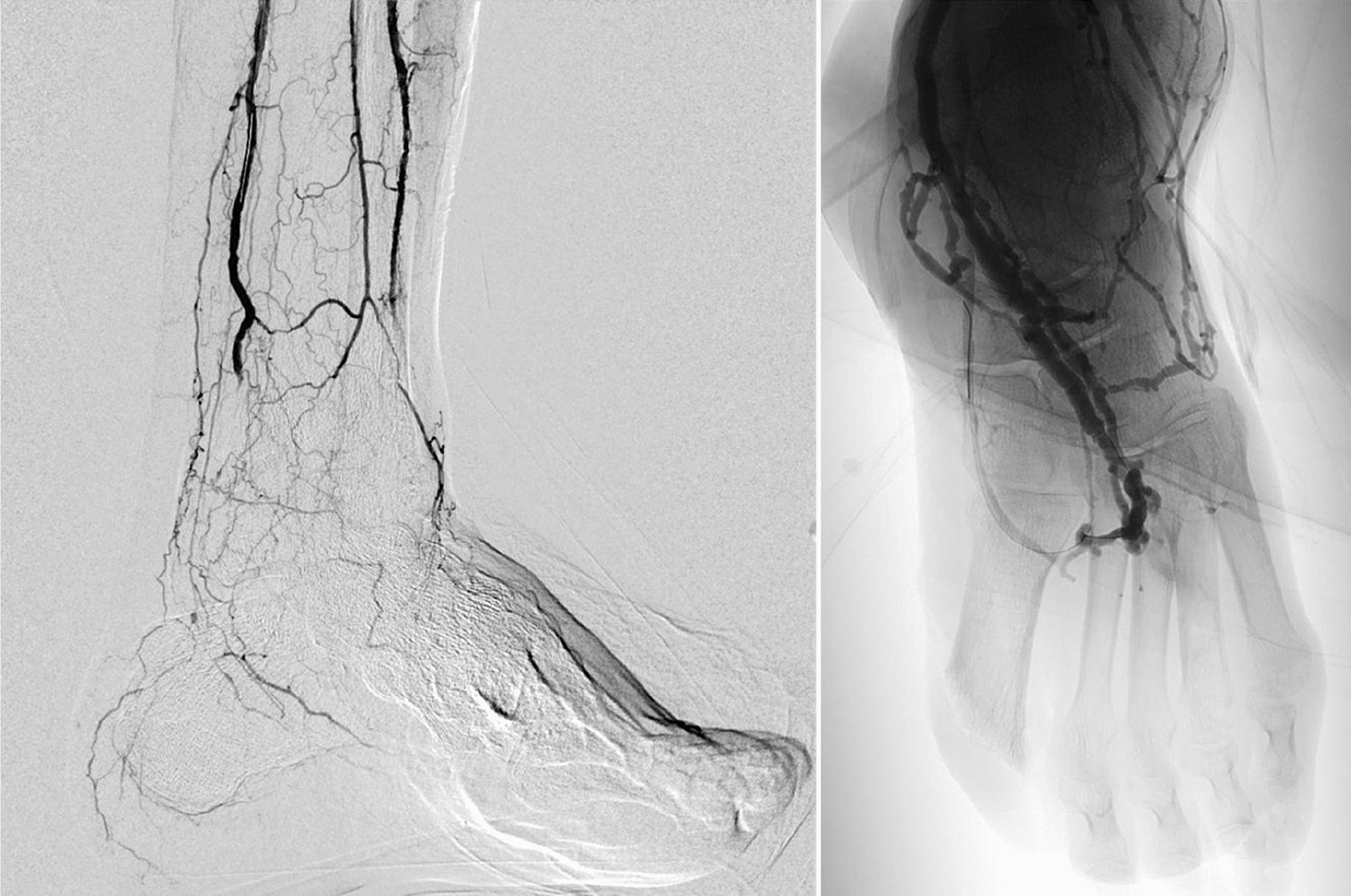
In our patient, the procedure was technically successful, with progressive improvement in local clinical parameters and transcutaneous oximetry values.
In many cases, the arterialization procedure is repeated to perform additional interventions or surgical revisions aimed at optimizing blood flow or managing complications, or to carry out complementary procedures if the clinical condition requires it. In this case, the optimal transcutaneous oximetry values demonstrated the clinical success of the single procedure, making repetition unnecessary.
The postoperative course was uneventful and led to complete re-epithelialization of the surgical site, with satisfactory functional recovery and maintenance of autonomous ambulation with assistance devices.
This clinical case highlights how this procedure may represent a limb-salvage strategy for patients with no vascular options.
It should be noted, however, that despite being an elderly patient, he did not suffer from heart failure or have a high bleeding risk.
Therefore, careful consideration must be given to multimorbidity, which may expose patients to procedural failure, as well as the need for intensive antiplatelet/anticoagulant therapy to prevent stent reocclusion, this poses an already elevated risk in elderly individuals.


Comments (0)