
Remember me

From January 11, 2020 to January 5, 2022, 121 residents were invited to participate and 71 (58.7%) responded favorably. Among those who agreed to participate, 24 out of 71 (33.8%) met the exclusion criteria, leaving 47 out of 71 (66.2%) eligible for the T0 survey. 35 out of 71 (49.3%) also responded to the T6 survey. Four participants started but did not complete T6, resulting in 31 complete profiles. Flow-chart is available in Fig. 1. The partial answers of these 4 participants were, however, included in the statistical analyses. Answers to the survey given by all participants are summarized in Appendix 2. Comparisons of results between inclusion at T0 and T6 are presented in Table 1. The statistical evolution of the main scales tested is shown in Fig. 2. Participant’s demographic characteristics are available in Table 2. Six outcomes remained significant under FDR correction.
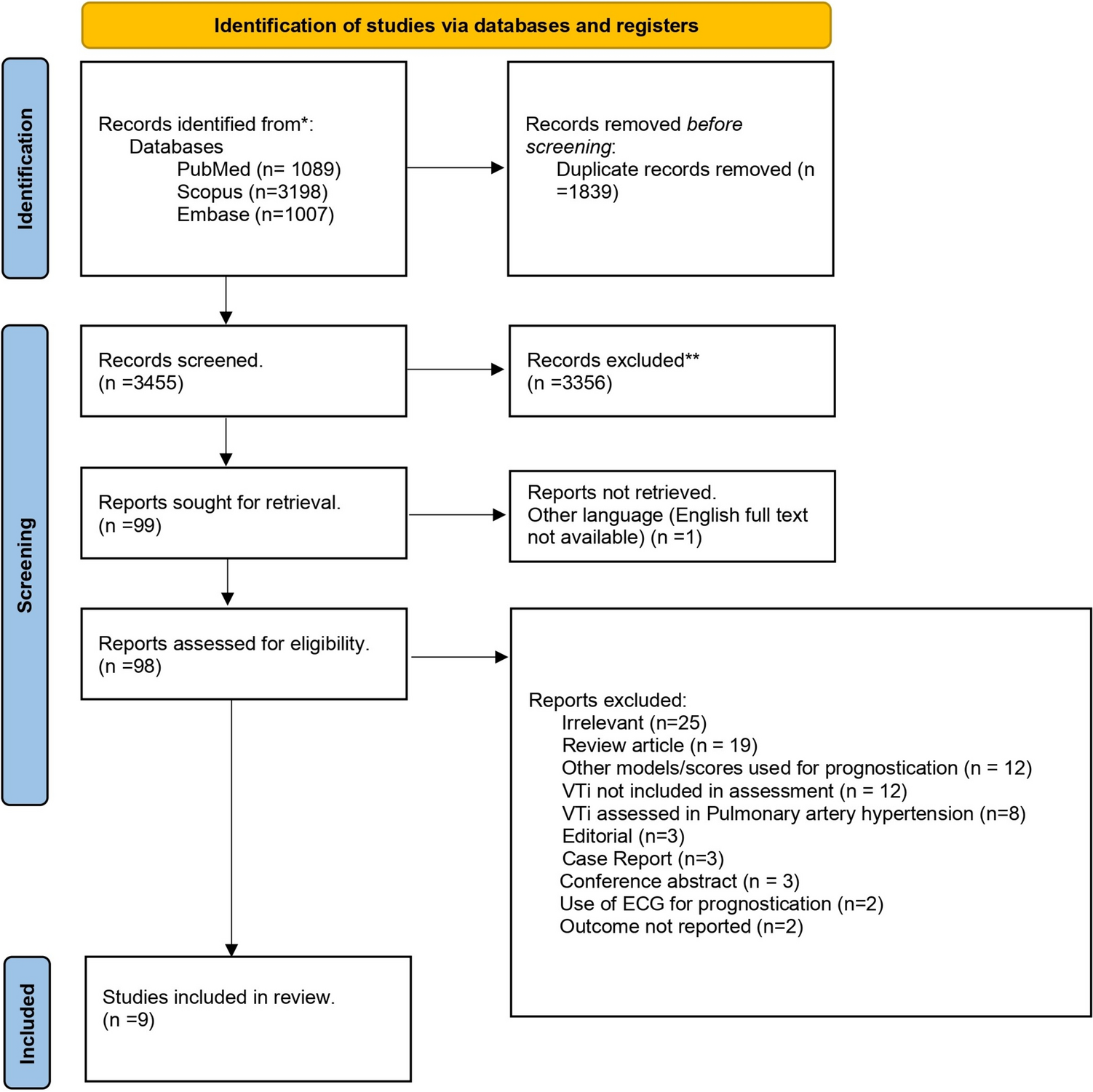
Fig. 1
Flow chart. T0, baseline survey; T6, 6-month follow-up survey
Table 1 Comparison of the various scores between T0 and T6Fig. 2
Evolution of quantitative analyses. Maslach Maslach Burnout Inventory score; HAD Hospital Anxiety and Depression Scale score; PSQI Pittsburgh Sleep Quality Index score; IPROF professional identity score; T0 baseline survey; T6 6-month follow-up survey
Table 2 Characteristics of the study population (n = 35) consisting of ED residents who completed both surveys, Lausanne University Hospital, 2020–2022Concerning the MBI subscale scores, emotional exhaustion (EE) increased (18, interquartile range [IQR] 10–24 vs. 21, IQR 16–28) after 6 months in the ED (p = 0.0259). High emotional exhaustion (≥ 30 points) was found in 5 out of 35 participants (14.3%) at T0 and 6 out of 35 (17.1%) at T6, the greatest individual increase being + 29 points. Depersonalization (DP) significantly increased (9, IQR 3–11 vs. 11, IQR 5–16) (p = 0.0064), with high depersonalization (≥ 12 points) in 8 out of 35 (22.8%) participants at T0 and 16 out of 35 (45.7%) at T6, the greatest individual increase being + 20 points. No significant difference in personal accomplishment was found between T0 and T6.
Regarding the HAD scale scores, the results showed that anxiety decreased after 6 months in the ED, despite identical median scores at T1 and T6 (6, IQR 5–10 vs. 6, IQR 4–8). Depression scores showed a slight but significant increase in median value (2, IQR 1–5 vs. 3, IQR 2–5) (p = 0.0185).
The PSQI scores indicated that sleep quality deteriorated over 6 months, with median scores increasing from 4 (IQR 3–5.5) to 5 (IQR 4–6) (p = 0.0022).
The Professional Self-Identity Questionnaire for health and social care professions showed a statistically significant increase in scores despite the same median score occurring at T0 and T6 (33, IQR 28–36 vs. 33, IQR 30–40) (p = 0.0046).
After 6 months, participants spent less time on personal development activities, averaging 8 (IQR 5–14) vs. 6 (IQR 4–10) hours per week. However, no significant changes were observed in alcohol, tobacco, medicine, or drug use, and the proportion of religious believers remained stable. 18 out of 31 participants (58%) showed minimal weight variation between T0 and T6 ( – 1.9 to + 1.9kg), the largest changes ranging from – 5kg (1 resident) to + 5kg (1 resident). At the first survey, 13 out of 31 residents (41.9%) had already consulted a mental health professional or were receiving follow-up care. By T6, this number had slightly increased to 14 out of 31 (45.2%).
Semi-structured interviews provided valuable insights into the unique aspects of emergency work and brought various subjects to light. A common stressor for participants was the pressure of patient flow. Although senior attending physicians oversee the management of overall flow, residents were highly concerned with waiting times and the number of patients in waiting rooms, and felt pressure to "move patients on." This pressure resulted in less time for each patient, inducing fear of medical errors and frustration from rushing their work. The lack of time sometimes led to a loss of empathy and reduced availability for therapeutic relationships. Overall, the pressure to manage flow contributed to a sense of practicing medicine that was misaligned with participants' values and beliefs.
The irregular working pattern had an impact on participants in various ways. Most felt out of sync with those around them, negatively affecting their social and family life. Some struggled with evening and night shifts, experiencing severe sleep issues (one participant had a car accident attributed to sleep deprivation). However, some participants appreciated the irregular rhythm and occasional weekdays off. Overall, irregular shifts were generally seen as negative, but there were notable exceptions.
Participants found emergency medicine's focus on diagnosing and treating acute problems satisfying. They appreciated the brief, punctual patient interactions, usually lasting a few hours. However, some were frustrated by the lack of involvement in patient follow-up during hospitalization. Overall, they valued the clinical aspects of emergency medicine, finding it more focused than was the case in other specialties.
Some participants shared deeply challenging emotional experiences in the ED, such as sudden unexpected deaths in young patients and breaking bad news in a rushed environment. These experiences did not cause major or lasting stress.
The ED ambiance was almost unanimously described as excellent and quite supportive. Participants appreciated the collaboration with the nursing team and with their peers, and they praised their supervisors as being highly competent, available, and very supportive.
Comments (0)