ACS classically present as a tightening-type chest pain on the left side, which may radiate to the neck, jaw, or upper limbs. However, atypical presentations are not uncommon, and diagnosing myocardial ischaemia in such scenarios requires a high degree of clinical suspicion. A thorough history and physical examination remain vital in identifying ACS, especially in patients with risk factors such as diabetes mellitus [12].
This case aligns with previously reported instances of cardiac cephalalgia, where headache was the primary symptom of acute coronary events. In a case series by Kobata et al., four patients exhibited similar presentations, with headaches preceding or coinciding with myocardial ischaemia. Notably, common cardiovascular risk factors such as hypertension, diabetes, hyperlipidaemia, and smoking were prevalent among these patients.
In a review of 30 cases, Wei and Wang found that patients commonly presented with migraine-like headaches, often located in the frontotemporal or occipital regions. In some cases, headache was the sole manifestation of ischaemia. The majority of patients were males over 50 years of age with typical cardiovascular risk factors. Headaches were frequently associated with autonomic symptoms, and electrocardiographic changes along with elevated cardiac enzymes supported the diagnosis. Importantly, symptom resolution followed appropriate coronary intervention in most cases.
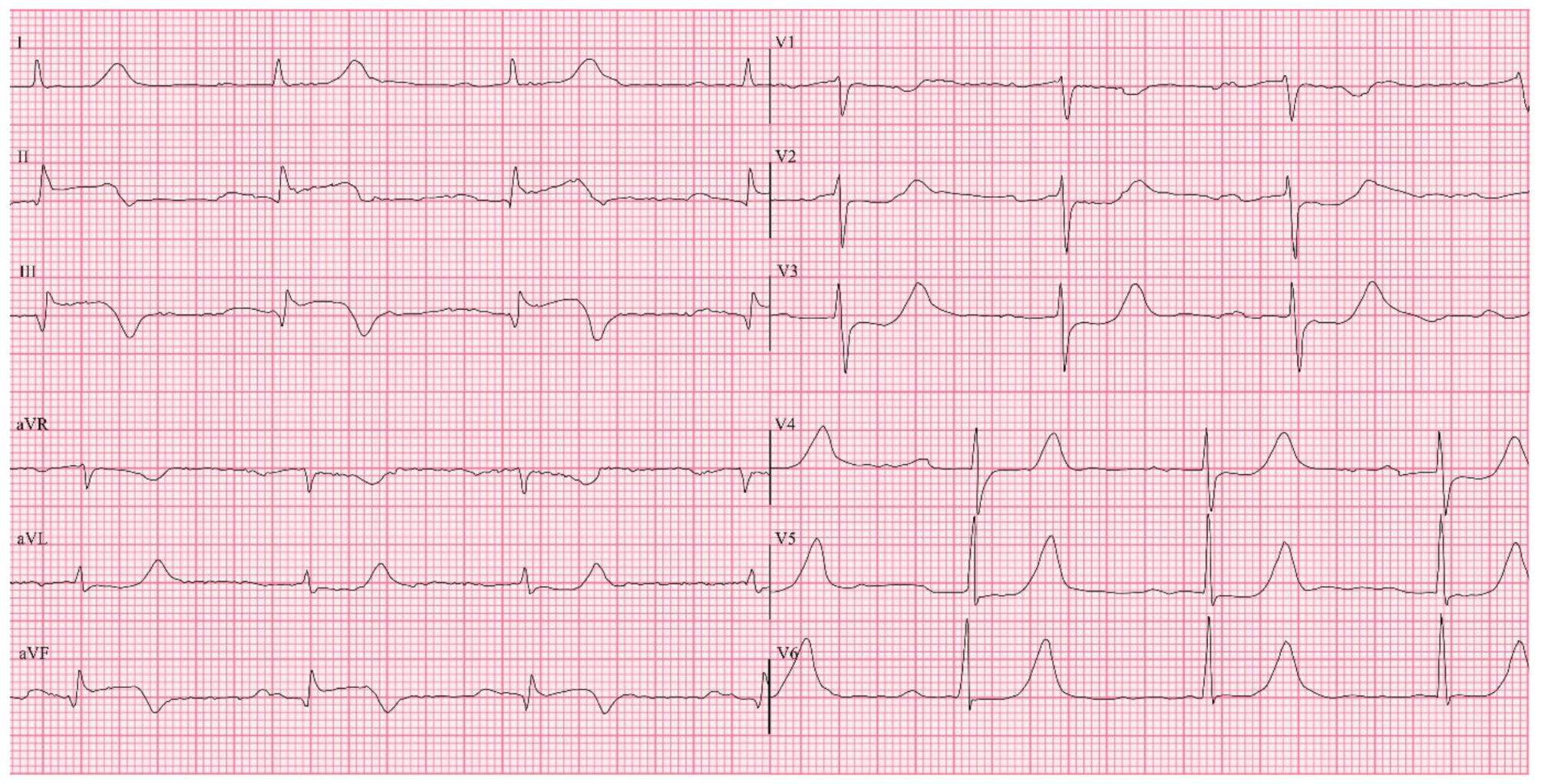
Our patient presented with a sudden-onset severe headache that awakened him from sleep, an unusual manifestation of ACS [13]. Although subarachnoid haemorrhage (SAH) is the most common life-threatening cause of sudden-onset severe headache, myocardial ischaemia should also be considered, particularly when the risk factors for ischaemic heart disease are present and typical intracranial causes are excluded. Ideally, a non-contrast CT brain should be the first step in excluding SAH [14]. However, in this patient, the presence of ECG changes and haemodynamic instability pointed to a diagnosis of STEMI, indicating that an urgent coronary intervention was necessary. The severity and onset of the headache ruled out a post-febrile headache, while the absence of focal neurological deficits, in combination with the ECG findings, supported the diagnosis of cardiac cephalalgia [15].
Cardiac cephalalgia is a rare presentation of myocardial ischaemia [3,4,5,6,7,8,9,10,11, 16]. According to the International Classification of Headache Disorders (ICHD-3), cardiac cephalalgia is defined as a migraine-like headache that is usually, but not always, triggered by exertion, occurs in the context of myocardial ischaemia, and is relieved by nitrates [15]. The diagnostic criteria for cardiac cephalalgia are summarised in [Table 1].
Table 1 Diagnostic criteria for cardiac cephalalgiaThis patient had several risk factors for coronary artery disease, including long-standing poorly controlled diabetes mellitus and a significant smoking history. Diabetes is associated with accelerated atherosclerosis and autonomic neuropathy, which may blunt the typical anginal symptoms and result in silent or atypical presentations such as fatigue, dyspnoea, nausea, abdominal pain, or rarely, headache [17].
Autonomic neuropathy leads to sensory denervation of the cardiac afferents, which may explain the absence of chest pain in diabetic patients with myocardial ischaemia. Histological studies have shown abnormalities in autonomic nerve fibres in such patients [18]. Imaging studies like m-Iodobenzylguanidine scintigraphy also support the theory of sympathetic denervation contributing to altered pain perception in diabetic patients [19]. Furthermore, the lack of a circadian pattern in myocardial events in diabetics suggests significant autonomic dysregulation [20, 21].
Distinguishing cardiac cephalalgia from migraine is particularly crucial. Triptans and ergot derivatives, often used to treat migraine, are vasoconstrictors and contraindicated in patients with myocardial ischaemia [15]. Hence, it is prudent to include ECG in the initial evaluation of patients presenting with acute headache, particularly in those with cardiovascular risk factors. Serial ECGs and cardiac biomarkers may further aid diagnosis [22].
The underlying pathophysiology of cardiac cephalalgia is not fully understood [7, 10, 11, 23]. However, several hypotheses have been proposed to elucidate its mechanism. One hypothesis involves the referred pain from convergence of afferent cardiac vagal fibres and afferent pathways of cranial pain fibres [7, 11, 24]. Another proposed mechanism implicates the release of proinflammatory neurotransmitters such as bradykinin, histamine, adenosine, and serotonin, during myocardial ischaemia, which may lead to cerebral vasodilation and subsequently provoke headache [24, 25]. A further theory suggests that headache may result from increased venous congestion as a consequence of acute heart failure following myocardial ischaemia [26].
In this patient, the referred pain mechanism seems plausible. His longstanding poorly controlled diabetes likely resulted in cardiac autonomic neuropathy, masking typical ischaemic pain while allowing alternative afferent pathways to mediate headache [27].
Interestingly, he had a recent history of upper respiratory tract infection (URTI) with throat irritation. URTIs are recognised triggers for ACS, particularly in the first two weeks following infection [28, 29]. The proposed mechanism involves inflammatory and pro-thrombotic processes that destabilise atherosclerotic plaques, increasing the risk of acute coronary events [28]. The patient had also received diclofenac sodium (50 mg twice daily), a non-steroidal anti-inflammatory drug (NSAID), for two days prior to admission. NSAIDs, especially diclofenac, are associated with increased cardiovascular risk and may precipitate ACS, particularly in patients with pre-existing cardiovascular risk factors [30,31,32].





Comments (0)