Study design and population
This study was conducted at Xijing 986 Hospital, Air Force Medical University between January 2021 to June 2023. We enrolled 300 adult outpatients with documented hypertension and elevated HCY levels (≥ 15 µmol/L), fulfilling the definition of H-type hypertension. The study protocol was approved by the Institutional Review Board of Xijing 986 Hospital, Air Force Medical University, and written informed consent was obtained from all participants prior to enrollment. Patient confidentiality was protected by assigning unique identifiers and restricting data access to authorized research personnel.
A prespecified protocol (Version 1.2, approved by the Institutional Review Board on 18 December 2020) defined the inclusion criteria, variables to be extracted, primary outcome, and the statistical analysis plan—including the single a-priori interaction test. The protocol was not prospectively registered but is available from the corresponding author on reasonable request.
Inclusion criteria
1), systolic blood pressure (SBP) ≥ 140 mmHg or diastolic blood pressure (DBP) ≥ 90 mmHg on at least two separate occasions, or current use of antihypertensive medication; 2), fasting HCY ≥ 15 µmol/L based on local laboratory reference ranges; 3), ability to provide written informed consent.
Exclusion criteria
1), known CKD stage ≥ 3b or on dialysis; 2), acute systemic illness, active infection, or inflammatory conditions that could spuriously elevate NGAL; 3), pregnancy or lactation; 4), severe hepatic dysfunction; 5), inability to comply with study procedures, including 24-hour ambulatory blood pressure monitoring.
Data collection
Participants meeting eligibility criteria were invited to undergo a baseline clinical assessment. Demographic information, medical history (including hypertension duration, comorbidities, and medication use), and lifestyle factors (e.g., smoking status) were recorded using a standardized questionnaire. Anthropometric measurements included height and weight for body mass index (BMI) calculation.
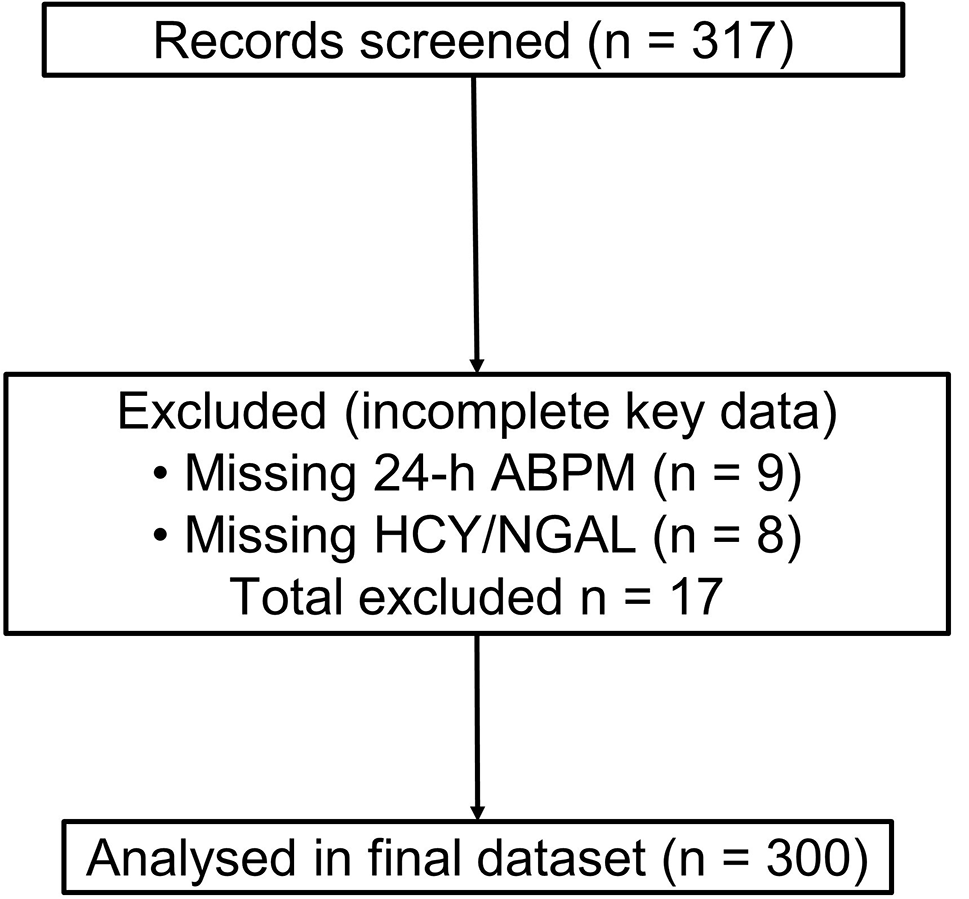
Of 317 screened records, 17 were excluded because either 24-h ABPM (n = 9) or laboratory measurements of HCY or NGAL (n = 8) were incomplete, leaving 300 participants with complete data on all primary and covariate variables. Because this was a retrospective audit of routinely collected data, all 300 consecutive eligible out-patients were included; no formal sample-size calculation was undertaken. For secondary covariates (folate, vitamin B12, smoking status), missingness was < 1%; these values were imputed with the sex-specific median (continuous) or mode (categorical).
Blood pressure variability assessment
Blood pressure was recorded using 24-hour ABPM (Mobil-O-Graph, I.E.M. GmbH, Stolberg, Germany). Cuff readings were obtained every 15–30 min during daytime and every 30–60 min overnight. Participants were instructed to maintain their usual activities but refrain from strenuous exercise and remain still during measurements. For each participant, the standard deviation of systolic blood pressure (BPV-SD) over the full 24-hour ABPM period was derived from valid recordings.
Coefficient of Variation (CV): A normalized measure of dispersion that accounts for differences in mean BP. CV was calculated by the formula:
$$} = }} \over }}} \times 100\% $$
Weighted Standard Deviation (wSD): Daytime and nighttime SD were separately calculated and then used a weighting factor proportional to the duration of each period to derive an overall wSD for the 24-hour period.
Average Real Variability (ARV): ARV was calculated by the formula:
$$} = }\sum\limits_^ }}_} - }}_k}} \right|} $$
To be included in the BPV analyses, each participant’s 24-hour ABPM recording had to meet a minimum threshold of 70% valid measurements across the entire 24-hour period. Specifically, for the daytime interval (6:00 AM–10:00 PM), participants were required to have at least 70% of scheduled readings successfully recorded, and the same criterion applied to the nighttime interval (10:00 PM–6:00 AM).
Of the 300 enrolled participants, 15 (5.0%) failed to meet this criterion on their first ABPM attempt due to technical issues or participant-related factors (e.g., device removal, excessive movement). These 15 individuals were asked to repeat the ABPM session within one week. Following this second attempt, all participants achieved the 70% threshold, each with adequate 24-hour ABPM data (Supplementary Table S1).
Laboratory measurements
After an overnight fast, venous blood was drawn and serum was isolated for the measurement of homocysteine, folate, vitamin B12, serum creatinine, and NGAL. The levels of homocysteine, folate, vitamin B12 and NGAL (Cat.#EHLCN2, Invitrogen. Analytical sensitivity: 4 pg/mL; Assay range: 4.1-1,000 pg/mL) were determined using commercial assay kits. Estimated glomerular filtration rate (eGFR) was calculated using the CKD-EPI formula, and serum creatinine was measured via an automated analyzer.
Statistical analysis
All data were recorded in a secure electronic database. Continuous variables were summarized as mean ± standard deviation (SD), while categorical variables were presented as frequencies and percentages. Bivariate correlations (Pearson or Spearman as appropriate) were used to examine relationships among homocysteine, BPV-SD, and NGAL. Multiple regression models were constructed to assess the independent effects of HCY and BPV on NGAL, adjusting for potential confounders (age, sex, BMI, eGFR). Because experimental data suggest a biologic synergy whereby hyper-homocysteinaemia amplifies blood-pressure-induced tubular stress, we specified a single, a-priori interaction term (HCY ≥ 25 µmol/L × BPV-SD) as the primary effect-modification test. To control type-I error in a modest sample, no other interaction terms were included in the main model. In exploratory sensitivity analyses we additionally tested HCY × sex, HCY × diabetes, and BPV-SD × age; none reached significance (all p > 0.10) and they are not presented further. Robustness was further examined by replacing the dichotomized HCY term with the continuous product HCY × BPV‑SD after centering both variables at their means. Statistical significance was set at p < 0.05, and analyses were performed using R (version 4.4).





Comments (0)