Our study is a prospective study with a relatively large sample size, aimed at analyzing the relationship between serum Hcy levels and all-cause as well as CVD mortality in patients with CVD. In our cohort study, we observed that elevated serum Hcy levels were associated with an increased risk of both all-cause mortality and CVD deaths. While the typical definition of high homocysteine levels is set at greater than 15 µmol/L, our analysis revealed a significant association between Hcy levels and the risk of all-cause mortality and cardiovascular death even at levels below 14.5 µmol/L and 14.6 µmol/L. This suggests that the impact of Hcy on these health outcomes can be observed at lower concentrations than the commonly accepted threshold.
Our research has reached conclusions consistent with previous studies, suggesting that elevated levels of Hcy are associated with an increased risk of all-cause mortality [17, 18]. A cohort study indicated that in the population with coronary heart disease, even when Hcy levels fell within the normal range, the mortality rate for this group increased by 1.9 times compared to the reference group. This finding underscores the potential benefits of maintaining lower Hcy levels for patients with cardiovascular disease [19]. Another study highlighted the vulnerability of elderly individuals, as high Hcy levels in the elderly were significantly associated with an increased risk of cardiovascular events, cardiovascular mortality and all-cause mortality [1.68 (95% CI 1.06–2.67), 1.97 (95% CI 0.95–4.29), and 2.02 (95% CI 1.26–3.24)]. It’s worth noting that this effect was not statistically significant in the female subgroup, emphasizing the need for further research to clarify the potential gender-specific impact [7]. However, in VISP research, a randomized double-blind trial, high dose vitamin therapy had no effect on the outcome measures of stroke, CHD events, or death [20]. One possible reason that the treatment was not effective may have been that patients enrolled in this study had levels of total Hcy that were too low to show a large effect. Another consideration is that a longer duration of treatment may be necessary. Therefore, we also focus on exploring the long-term prognosis of higher levels of Hcy.
As previously mentioned, numerous studies have demonstrated a dose-response relationship between Hcy levels and the risk of mortality. Each 5 µmol/L increment in Hcy is significantly associated with an increased risk of all-cause and CVD mortality [6, 17]. The underlying pathophysiological mechanisms are intricate and multifaceted. One such mechanism involves the direct toxicity of Hcy on tissues, which can result in various detrimental effects, including oxidative stress, smooth muscle cell proliferation, the formation of reactive oxygen species, and the induction of unfolded protein responses [21,22,23]. These effects can contribute to the development of atherosclerosis, a major contributor to CVD [24]. On the other hand, homocysteinemia is also associated with the metabolic deregulation of the methionine cycle, leading to an imbalance between the biosynthesis and catabolism of Hcy [25]. This imbalance is linked to an increased risk of CVD, stroke, and myocardial infarction through mechanisms such as atherosclerosis, thrombosis, endothelial cell dysfunction, and oxidative stress [26, 27]. Another critical factor is the role of B vitamins in Hcy metabolism. Vitamin B and folate serve as important cofactors in Hcy metabolism, and an insufficient dietary supply of these nutrients can result in homocysteinemia [17, 28, 29]. Additionally, homocysteinemia can stimulate procoagulant factors and suppress anticoagulant factors, thereby enhancing thrombotic events [24, 30, 31].
We conducted further analysis and literature review regarding confounding factors in our study, which included age, gender, smoking, hypertension, diabetes, chronic kidney disease and serum vitamin B12 levels. A study involving 7872 subjects from the general population of China found that the Hcy level was significantly higher in males than in females in each age range [32]. Factors such as exposure to environmental cigarette smoking and alcohol consumption, genetic variation of methylene tetrahydrofolate reductase (MTHFR), and rates of re-methylation and transmethylation of Hcy may contribute to sexual differences in Hcy levels [33]. Our study revealed that Hcy posed a risk for both CVD death and all-cause mortality, and this risk was consistent across genders. Importantly, the degree of risk did not exhibit a statistically significant difference between the two gender groups. Elevated Hcy levels can lead to endothelial injury and smoking can exacerbate endothelial dysfunction by promoting oxidative stress and inflammation [34, 35]. Meanwhile, smoking is associated with lower levels of B-vitamins which are crucial for the metabolism of homocysteine [36]. The interaction between smoking and Hcy may enhance vascular inflammation and thrombus formation. The interaction between smoking and Hcy may enhance vascular inflammation and thrombus formation, leading to more severe cardiovascular conditions and ultimately higher mortality rates [34].
A cross-sectional study of the general population of China found that Hcy levels significantly increased after 50 years of age [37]. High levels of Hcy have been linked to the development and progression of age-associated disorders, including cardiovascular diseases, neurodegenerative disorders, and chronic kidney disease [38, 39]. It is important to acknowledge that the outcomes were negative in the age group of less than 60 years. This is likely attributable to the limited follow-up time, which resulted in a lower rate of endpoint events in this specific age group.
Hyperhomocysteinemia emerged as a risk factor for both all-cause mortality and cardiovascular death in both the smoking and nonsmoking groups. Notably, the elevated risk of cardiovascular death attributed to hyperhomocysteinemia was significantly greater in the smoking group when compared to the nonsmoking group, indicating that risk is further amplified in individuals who smoke [18]. Another study found that smokers with a plasma homocysteine level above 12µmol/L had a 12-fold increased risk of cardiovascular disease compared to non-smokers with normal plasma homocysteine levels [40].
In our study, we observed a higher proportion of hypertension among patients with elevated Hcy levels. One proposed mechanism for this association involves arteriolar constriction, renal dysfunction, increased sodium reabsorption, and heightened arterial stiffness [41]. Some studies have suggested that lowering Hcy levels with B vitamins can be an effective means of reducing blood pressure, especially in the management of drug-resistant hypertension [42]. Compared to the non-hypertensive group, Hcy was associated with a higher risk of all-cause mortalityd and CVD death in the hypertensive group, although no statistically significant differences were demonstrated. The relationship between Hcy and diabetes, particularly type 2 diabetes mellitus (T2DM), is complex. Some studies have found a positive association between elevated Hcy levels and T2DM, while others have found a negative association [43, 44]. In terms of diabetes complications, elevated Hcy levels have been associated with an increased risk of diabetic retinopathy [45].
Our study identified homocysteine Hcy as a risk factor for all-cause mortality irrespective of the presence of renal insufficiency. Hcy levels emerge as a consistent risk factor for both all-cause mortality and CVD mortality, irrespective of renal function.
Vitamin B12 is involved in the metabolic pathway that converts Hcy to methionine, an essential amino acid. This conversion process is catalyzed by the enzyme methionine synthase, which is dependent on Vitamin B12 [46]. Therefore, a deficiency in Vitamin B12 can lead to increased Hcy levels, leading to an increased risk of cardiovascular diseases [47]. In our study, we did not observe a statistically significant difference in the increased risk of cardiovascular death among individuals with higher vitamin B12 levels, implying that vitamin B12 supplementation might be considered an effective approach for reducing the risk of cardiovascular death.
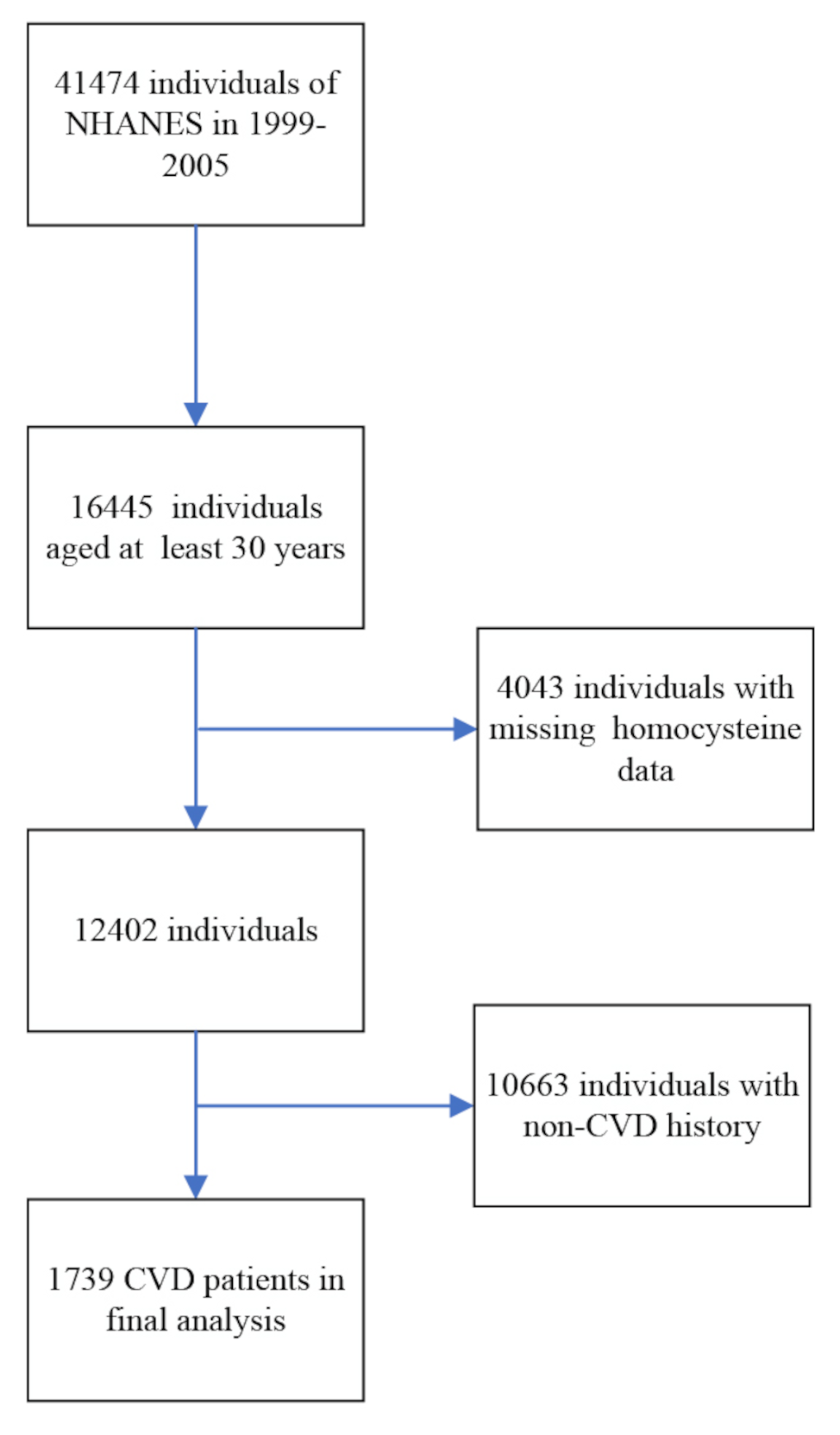
Nevertheless, it’s essential to recognize certain limitations in our study. Our research is based on a cross-sectional observational design, which allows us to establish a correlation between Hcy levels and CVD risk but falls short of establishing a definitive causal relationship. While we can observe an association, causation cannot be implied. Furthermore, the limitations of the NHANES database, which provides data at specific time points, make it challenging to determine the precise temporal relationship between Hcy levels and the risk of mortality. A more comprehensive assessment of temporal relationships would necessitate longitudinal data with multiple time points. Additionally, in Table S1, we compared the groups with missing data and those included in the analysis. The results showed significant differences in age and mortality, but no significant differences in other aspects. This may introduce some selection bias into our study.
Our findings imply that Hcy levels might serve as potential predictors of all-cause mortality and CVD mortality. It is plausible that Hcy testing could be incorporated into clinical practice to assess cardiovascular risk and predict mortality. Additionally, tailored Hcy management strategies based on individual patient characteristics could be developed. Further research can delve into the pathophysiological mechanisms underlying the relationship between Hcy and CVD. Prospective clinical studies could be conducted to elucidate the causal relationship between Hcy and the risk of CVD. This could provide valuable insights into preventive and therapeutic strategies for cardiovascular diseases.





Comments (0)