The majority of geriatric patients was found to have a very high fracture risk, accompanied by cognitive impairment, limitations in ADLs, highest level of care, number of diagnoses, and risk-factors highlighting the vulnerability of this group. Even though contraindications were present, specific-anti osteoporotic medication can be found for almost every geriatric patient.
Distribution and characteristics of very high-risk and high-risk patients
Even though European-wide estimations identified on average, only 18% of the population to be at high-risk or very high-risk (2); in our study population, a much higher proportion of 75% was found. As one major difference between the studies is the average age of the included participants (European-wide estimations, 50 years or older (2); our study population, 82 ± 7 years) and the included population (European-wide, total population aged 50 years or older; our study population, geriatric cohort), our results highlight the striking fracture-risk (5, 13) and increased demand for specific anti-osteoporotic treatment in geriatric patients (10, 14). In another cohort of geriatric day care patients, we observed similar prevalences (15). Likewise, Hadji et al. reported a significant increase in osteoporosis prevalence among older adults (16), although their reported prevalence was notably lower than in our cohort. As their data stem from German insurance records, this may reflect widespread under-diagnosis in the general population (16). In contrast, our data mainly come from geriatric clinic patients, likely representing a population with a higher disease burden and thus higher osteoporosis prevalence. This becomes even more apparent when taking into account that the majority of our geriatric study population, in particular 54%, were allocated to the very high-risk group in which the fracture-risk is most striking and therefore highly effective treatment is required (5). Nevertheless, only 36% of the total study population already had any type of specific anti-osteoporotic treatment listed as a regular medication. Of note, not only 72% of all included women were allocated to the very high-risk group for which our results support female sex as a major risk-factor (5, 13, 17) but also 20% of the included men were identified to be at very high-risk (20%), so that the fracture-risk must also not be underrated especially in aged men (18).
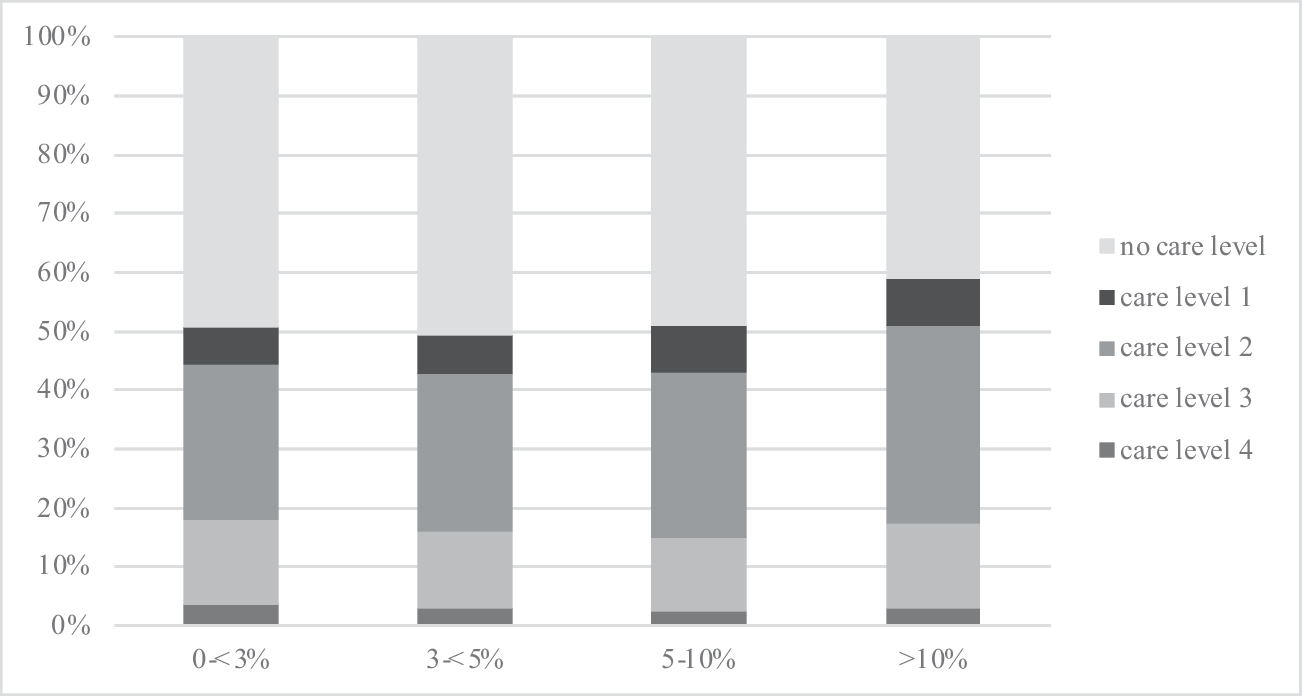
Even though in our study cohort mild cognitive impairment was present in all fracture-risk groups, patients in the very high-risk group had the lowest MMSE-score. Since cognitive impairment is known to increase the risk for complications and mortality after hip fractures, but is not included as a risk-factor for fracture risk calculation, screening for cognitive decline is highly recommended, especially in very high fracture risk patients (19). Additionally, also physical limitations in, e.g., ADLs—also not included in the fracture risk calculation—were mostly present in the very high-risk group leading to a loss of independency accompanied by the need for help when living at home or institutionalized (20, 21). In line with these findings, the percentage of patients with any care level also increased with increasing fracture-risk. Osteoporosis and osteoporotic fractures therefore still pose a huge socioeconomic burden as it is known that most of the money spent on osteoporosis is not spent on primary prevention but on the treatment of its consequences, including hospitalization and institutionalization (22). However, even in the very high-risk group, care level 2 was the most common care level indicating some preserved activity, and along with that an increased risk for falls and consecutively fractures. Since falls are well known to significantly increase the overall fracture risk, and data from the DUBBOS study population also demonstrated the substantial impact of falls on hip fractures, this finding particularly emphasizes that timely initiation of treatment is especially beneficial for older patients at very high risk (23, 24). In line with this, bone anabolic treatment for example has been shown to be most efficient and cost-effective especially in very high-risk patients (25,26,27). Interestingly, even though polypharmacy was evident in all fracture-risk groups, patients in the very high-risk group took on average one regular medication less than patients in the other fracture-risk groups but on the other hand had on average one more diagnosis and risk-factor. A risk–benefit-based prioritization of drugs or a reduction of fall-increasing drugs in multimorbid patients might be possible explanations for the difference in the number of regularly taken medications between the fracture-risk groups. But also, Ageism-related reasons leading to a less conscious prescription could be a possible explanation (28).
Contraindications for specific anti-osteoporotic/bone anabolic treatment
The majority of our study population was allocated to the very high-risk group for which, also in many other guidelines (25, 29), bone anabolic treatment is recommended (10). The striking demand for these medications especially in geriatric patients becomes apparent. As clinicians might worry about the applicability of bone anabolic agents in geriatric patients with regard to potential contraindications, we investigated the percentage of patients with a contraindication for bone anabolic- and antiresorptive treatment (7, 30). In 19% of the women and 8% of all patients from the very high-risk group, contraindications for Romosozumab or Teriparatide were found, respectively. Notably, impaired kidney function was the most common contraindication for Teriparatide use in our analysis. Still, even though only limited data are available, they suggest that even in severe cases, Teriparatide can improve bone density without worsening kidney function or increasing adverse events (31). It is also worth noting that the proportion of patients with contraindications for Teriparatide was likely underestimated, as certain factors, such as a history skeletal irradiation, could not be assessed due to limitations in the survey methodology (32). Using breast carcinoma in women and prostate carcinoma in men aged 80 years or older as surrogate parameters for a history of radiation therapy—since they are the most frequent cancers and typically require radiation therapy—their prevalence in 2022 was estimated at 23.8% and 26.3%, respectively, according to the International Agency for Research on Cancer (33). Therefore, the actual percentage of patients with a contraindication to Teriparatide might rather be approximately 30% (31). For Romosozumab, prior myocardial infarction or stroke was the most common contraindication. While the FDA (Food and Drug Administration) limits this to events within the past year, the EMA (European Medicines Agency) considers any such history a contraindication (34, 35). As our study followed EMA guidelines, all patients with an ICD-10 code for MI or stroke were included for contraindication calculation. Due to missing data on event timing, a comparison with FDA criteria was not feasible. The EMA also advises assessing overall cardiovascular risk, recommending use only after careful risk–benefit evaluation (34). Still, as Romosozumab is not renally eliminated, it has proven safe across varying kidney function levels, making it suitable for older patients (36).
However, even if the actual percentage of patients with a contraindication is underestimated, many geriatric patients will still be eligible for bone anabolic therapy.
As an alternative medication for the very high-risk- and first-line treatment for the high-risk group (10) for Denosumab, as confirmed by other authors, hardly anyone had any contraindications (37). This is most likely due to its non-renal elimination, making it a very suitable medication especially for geriatric patients in whom an impaired kidney function often is present (37,38,39). On the contrary, for bisphosphonates, a reduced kidney function poses a potential contraindication (40). In line with results of a population-based kidney-function study, only in 7–8% of the study population an impaired kidney function (defined as a glomerular filtration rate < 30 ml/min/1.73 m2 ≙ ICD-10 N18.3) was identified as a contraindication for bisphosphonate use (41). MR-ONJ is a dreaded but rare complication but if present poses a contraindication for antiresorptive treatment (42). However, in only a very small number of patients (0.4–0.5%), MR-ONJ was identified as a contraindication, reflecting its insignificant role in osteoporosis therapy (43).
With regard to the number of patients suitable for specific anti-osteoporotic treatment in the overall analysis, only a vanishingly small percentage (0.04–0.05%) of all patients requiring specific anti-osteoporotic treatment had a contraindication for all of the investigated medications (bisphosphonates, Denosumab, Romosozumab, and Teriparatide). Furthermore, more than 70% had no and approximately 20% only had a contraindication for one of the potential medications of which we concluded that suitable anti-osteoporotic medication can be found for almost every patient.
Limitations
The analysis of a large geriatric population from different geriatric institutions provides a good real-world description of the patients geriatricians deal with in their daily work in hospitals, day care clinics, and rehabilitation facilities. However, this approach means that the data do not represent a cross-section of the overall population of higher age. Secondly, the evaluation of the risk-factors and contraindications had to be based on retrospective analyses using ICD-10 and ATC-Codes leading to an underestimation of the risks and contraindications due to a lack of the reported data (e.g., limitations in kidney function were subsumed to levels of chronic kidney disease (CKD) as reflected in the ICD-10 codes and were not extracted from laboratory measurements). When timing of diagnosis, medication details (e.g., glucocorticoids), or fracture severity were relevant for risk calculation, the most conservative assumption was used due to missing duration data (e.g., as described in 2.3 if a type 2 diabetes mellitus was present in a patient the lowest numerical risk according to the duration (5–10 years, 1.1; > 10 years, 1.6) had to be applied). Although recent fractures indicate an imminent fracture risk, their timing could not be assessed, as this information was not included in the dataset. Additionally, risk-factors and contraindications that were not included in the geriatric assessment or routine data query such as “hip fracture of the parents” and “history of skeletal irradiation” could not be captured. Falls, a key fracture risk factor, could not be considered due to missing data, despite their strong link to imminent fracture risk. Similarly, the lack of BMD data limited the accuracy of risk estimation, as its omission can alter fracture risk gradients (44). For the identification of the number of patients suitable for any anti-osteoporotic treatment, no difference between the recommendations for each fracture risk group or female/male gender was made. As in 2017, the care levels in Germany were adapted; data had to be merged (also see supplement Table 3). Also, as data were mainly drawn from inpatient geriatric rehabilitation, to which patients with a very high care level usually are no longer transferred, none of the patients had care level 5 and the portion of patients with care level 4 was very small. Even though we filtered the data set for participants with preferably complete data on the interested variables, an underreporting of diagnoses or medications by the registering hospital, but also bias of included patients, cannot be excluded. For the evaluation of contraindications, contrary to daily clinical practice, we were not able to include aspects, such as intolerances against specific medications, or the patient’s preference regarding the application type or simply the fact that especially bone anabolic treatment is not started during hospital stay due to financial issues. As our study identified a relatively high portion of geriatric patients potentially requiring bone anabolic treatment, one might fear huge expenses for the healthcare institutions. However, one has to consider that our study included highly selected geriatric patients treated at geriatric institutions and therefore not representing the total population at this age. Especially, in this group of patients, the usage of bone anabolic treatment is probably rather cost-effective as they have been demonstrated to prevent many fractures and therefore safe costs for the healthcare system. Nevertheless, a personalized drug-prescribing process is still needed as some geriatric patients (e.g., with a longer life expectancy and high quality of life) might benefit more than others (e.g., highly care-dependent patients with a reduced life expectancy).


Comments (0)