Hip fractures are the most serious form of fragility fractures, and despite advances in modern medicine, mortality rates remain high. The costs of a hip fracture are also substantial, with health and social care costs at US$ 43,669 at 12 months [17]. To improve clinical outcomes and quality of life for hip fracture patients, many initiatives have been established, including orthogeriatric co-care, multidisciplinary care teams and fracture liaison services [2]. During in-patient stay, pre-operative and post-operative, blood taking for monitoring is often performed. This study aimed to provide pragmatic data and analysis to aid in the prediction of mortality for hip fracture patients at 1-year post-operation.
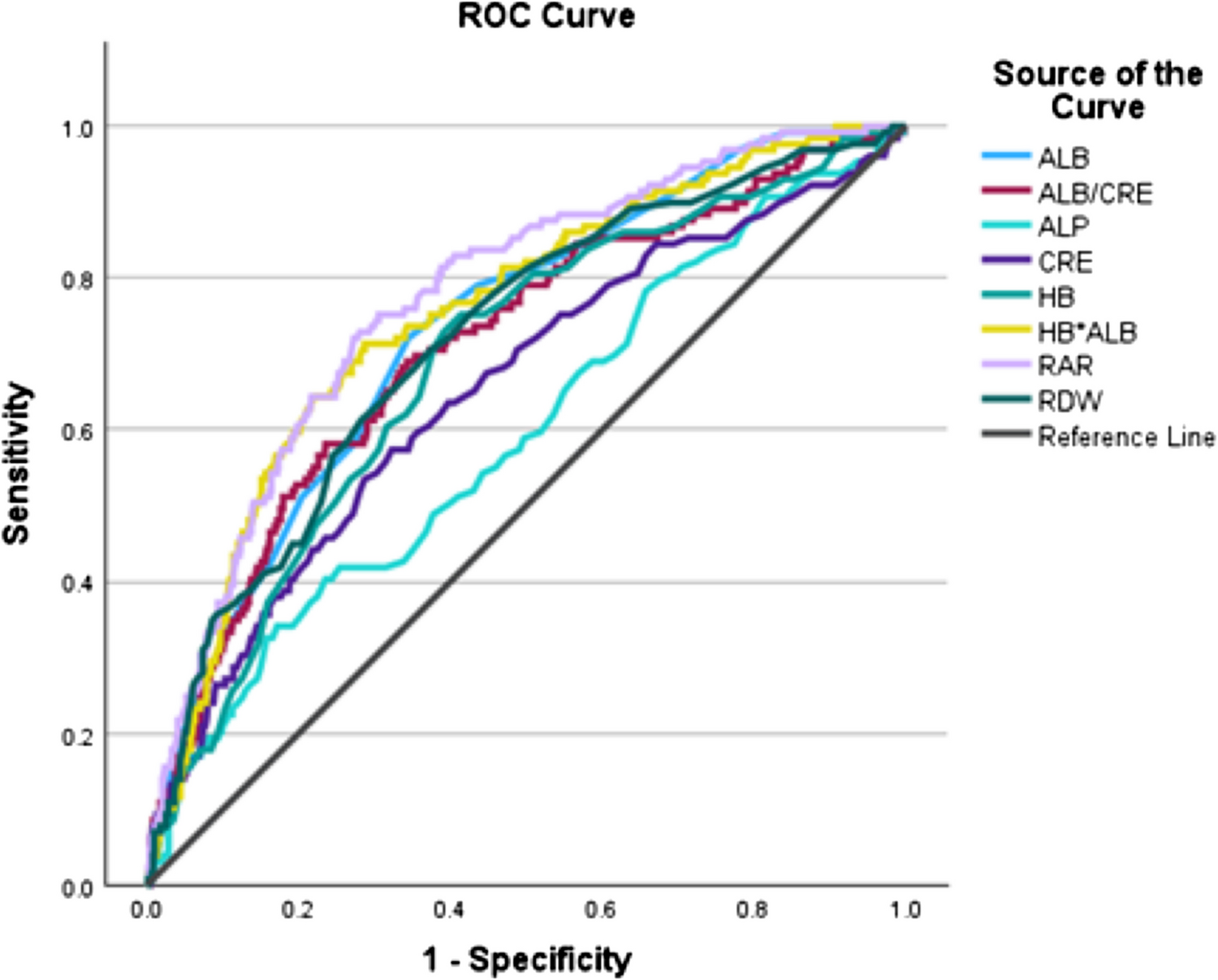
Our study establishes AHI as a potential novel predictor of 1-year mortality in elderly hip fracture patients. ROC analysis demonstrated AHI’s strong prognostic accuracy for 1-year mortality, with a preoperative cut-off value < 3331, which predicted nearly four times increased risk of 1-year mortality in our adjusted hazard model, indicating the potential utility in clinical settings. AHI’s performance is notable given its simplicity, combining two routine preoperative parameters—albumin and haemoglobin, both widely available in clinical settings. However, AHI’s AUC overlap with that of albumin alone (AUC: 0.73, 95% CI: 0.69–0.78), suggesting that while AHI offers strong prognostic performance, its improvement over albumin alone may not differ much. AHI’s advantage lies in its ability to combine two markers, providing a more comprehensive assessment of nutritional status. Pre-operative parameters generally showed significant predictive value, highlighting their importance in early risk assessment in a fracture liaison service. Previous studies have also shown that anaemia and hypoalbuminemia are manifestations of poor nutritional status and are risk factors for poor outcomes in other diseases, including stroke [18], gastrointestinal surgery [16], and cardiovascular disease [19]. Furthermore, the use of systemic immune-inflammation markers, including peripheral platelet, neutrophil, and lymphocyte counts, has also been analysed as prognostic markers. However, it is also noted that impairment of the immune system from chronic diseases may lead to unpredictable effects and may not be modifiable [20].
The main parameters that were found to have increased risk of mortality at 1-year post-operation were anaemia, hypoalbuminemia, raised creatinine, and increased albumin/creatinine ratio. Routine monitoring of these blood parameters helps identify high-risk patients early, enabling targeted interventions including nutritional support, anaemia management, and renal function monitoring to improve patient outcomes and reduce mortality. For instance, based on our findings, patients with AHI < 3331 may benefit from pre-operative optimisation strategies. Our new finding of AHI as a good predictor of mortality can lead to further initiatives and the finding of solutions to decreasing hip fracture mortality. Orthogeriatric co-management of hip fracture patients has been advocated due to better outcomes, including decreased time to surgery, improved clinical management and reduced 1-year mortality [21]. A previous systematic review and meta-analysis also showed that orthogeriatric care models reduce length of stay, in-hospital mortality and delirium of hip fracture patients, together with reduced complications and costs [22]. Cox hazard models also showed AHI’s predictive consistency at 3 months (HR: 4.00, 95% CI: 2.04–7.84) and 6 months (HR: 3.56, 95% CI: 2.20–5.77), supporting its broader utility across time points (Table 3). Optimising patients pre-operatively and post-operatively, as well as monitoring and intervening in blood parameters and holistic care, may be effective in reducing mortality. However, there are yet to be randomised controlled trials to show which orthogeriatric care models are most effective.
We evaluated AHI’s performance against red cell distribution width (RDW) and RDW/albumin (RAR) to determine if AHI is better or equivalent to these markers for 1-year mortality prediction. ROC analysis showed RAR had the highest AUC for 1-year mortality (0.77, 95% CI: 0.73–0.82) with adjusted hazard ratio (HR: 3.94, 95% CI: 2.62–5.90), slightly outperforming AHI (AUC: 0.75, 95% CI: 0.71–0.80; adjusted HR: 3.67). RDW had a lower AUC (0.72, 95% CI: 0.67–0.77) with HR (2.12, 95% CI: 1.43–3.14), indicating that AHI is superior to RDW as a prognostic marker for 1-year mortality. The overlapping confidence intervals of AHI and RAR suggest their prognostic performance was comparable, though RAR’s higher HR indicates a stronger association with 1-year mortality. RAR’s performance reflects its ability to capture both anaemia and inflammation, as RDW is a marker of systemic inflammation and albumin reflects nutritional status [18, 19]. However, AHI’s simplicity, requiring only albumin and haemoglobin, makes it accessible for routine clinical use compared to RAR, which requires an additional parameter of RDW. Furthermore, AHI’s direct focus on malnutrition-related factors may offer a more targeted approach for interventions in elderly hip fracture patients, where nutritional deficits are a primary concern contributing to 1-year mortality.
The strengths of this study include the large cohort and a robust AUC for AHI in predicting 1-year mortality via ROC analysis, and comprehensive Cox models that confirm its predictive value at 1 year, with additional consistency at 3 and 6 months. The inclusion of RDW and RAR provides a thorough comparison, reinforcing AHI’s utility for 1-year mortality prediction. However, AHI primarily reflects preoperative poor nutritional status, and dietary interventions post-hip fracture may not rapidly reduce mortality, as some elderly may have a chronic nature of malnutrition. However, preoperative identification of high-risk patients using AHI could still potentially give earlier interventions, such as nutritional optimisation before elective surgeries or in high-risk patients, and inform orthogeriatric co-management strategies, potentially improving outcomes over time. Interestingly, previous pre-clinical studies have also shown that osteoporotic fracture healing may be compromised [23, 24], and clinical studies have also shown an association with non-union [25]. Therefore, research has also been performed on how to accelerate bone union [26, 27]. Nutrition is also an important aspect for fracture healing [28], and further studies can assess this as an outcome as well. Additional studies should test the modifiability of AHI through targeted interventions. Limitations in our study include unmeasured confounders (e.g., frailty indices) and the lack of intervention data to assess AHI’s direct impact on outcomes.


Comments (0)