
Remember me
For acute ischemic stroke (AIS) and intracerebral hemorrhage (ICH), research suggests that as blood pressure variability (BPV) increases, clinical outcomes worsen [1,2,3,4,5,6]. Higher BPV is associated with recurrent stroke [1], symptomatic intracranial hemorrhage after endovascular therapy [4], and increased disability and death at 90 days [2, 3, 5, 6]. Despite this association, no consensus exists for a definition of BPV in AIS, ICH, or for BPV targets. In 2022, the American Heart Association (AHA)/American Stroke Association (ASA) guidelines in spontaneous ICH recommended “maintaining smooth, sustained blood pressure control, avoiding peaks and large variability” to improve outcomes after ICH (class of recommendation: 2a; level of evidence: B, nonrandomized) [7]. For ICH associated with acute hypertensive response (systolic blood pressure [SBP] 150‒220 mm Hg), AHA/ASA guidelines recommended a target SBP of 140 mm Hg with maintenance SBP of 130‒150 mm Hg [7]. No recommendation is provided for baseline SBP > 220 mm Hg. The guideline also emphasizes expedited care, noting that blood pressure (BP) treatment within 2 h of ICH and reaching BP targets within an hour may improve functional outcome (class: 2a; level: C, limited data) [7]. The European Stroke Organisation acknowledges that benefits and risks of intensive BP lowering on outcomes remain uncertain after acute ICH [8]. In hyperacute ICH, the European Stroke Organisation recommends lowering SBP below 140 mm Hg to reduce hematoma expansion, but keeping it > 110 mm Hg and avoiding SBP drop > 90 mm Hg (quality of evidence: moderate; strength of recommendation: weak) [8].
For AIS, the 2019 AHA/ASA Guideline recommended maintaining BP < 180/105 mm Hg for ≥ 24 h after intravenous thrombolysis (IVT) but did not offer BPV recommendations [9]. Specific SBP goals after IVT were not provided from the cited Enhanced Control of Hypertension and Thrombolysis Stroke Study (ENCHANTED) trial, in which 90-day outcomes were similar for patients with SBP targets < 180 mm Hg versus 130–140 mm Hg [9, 10]. Thus, practice guidelines recommend “smooth” and “sustained” BP control in acute ICH, guideline recommendations for both ICH and AIS remain nonspecific [5, 7], and evidence supporting specific SBP targets is limited.
Because this BPV quandary remains unsolved, we convened the Blood Pressure Variability in Cerebrovascular Emergencies (B-PRECISE) Consortia, an invited group of seven experts (all authors of this article) in vascular neurology, neurocritical care, perioperative medicine, emergency medicine, and clinical pharmacy. We met in person before the International Stroke Conference in Phoenix, Arizona in February 2024. Follow-up meetings occurred virtually, after Consortia members reviewed and edited drafts of the proceedings. This consensus is based on the current (limited) literature and collective decades of multidisciplinary clinical experience. Discussion questions raised by the Consortia (Table 1) had the ultimate goals to: initiate evidence-based dialogue about BPV; stimulate future research strategies on post-stroke BPV; and, similar to “CODE ICH” standardizing ICH hyperacute treatment [11], recognize that post-stroke BPV management represents an unmet need ripe for standardization.
Table 1 Discussion questions at the Blood Pressure Variability in Cerebrovascular Emergencies Consortia meetingBPV and Stroke OutcomesEvidence of a relationship between BPV and poor functional outcomes derives mostly from prospective cohort studies and post hoc analyses of randomized controlled trials (Table 2 and Supplement) [12,13,14]. The Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial 2 (INTERACT2) and Antihypertensive Treatment of Acute Cerebral Hemorrhage 2 (ATACH-2) failed to demonstrate significant associations between intensive SBP control and 90-day functional outcomes or death after ICH, but suggested that greater BPV may result in neurological deterioration and worse functional outcomes [15, 16].
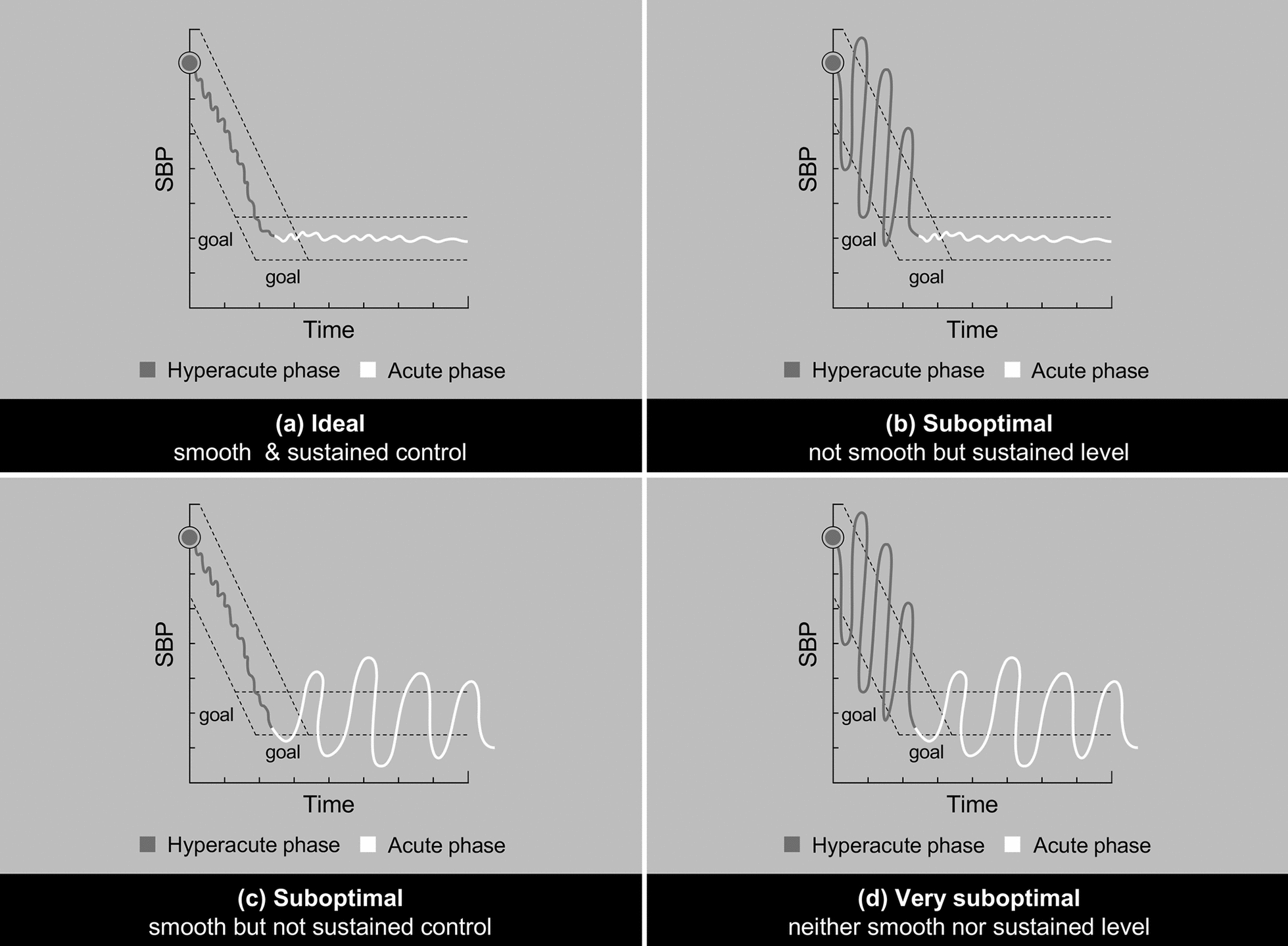
Table 2 Select studies evaluating BPV in ICH (above) and AIS (below)Proposing a Practical Definition of BPVStudies that examined BPV have used various definitions of BPV and a panoply of BPV endpoints (Table 2). Knowledge gaps exist because: (1) BPV is not yet practically defined or routinely assessed; (2) BPV goals may require tailoring to specific clinical scenarios; and (3) pharmacological options to minimize BPV have not been thoroughly, formally evaluated. Therefore, the Consortia proposed a practical definition of BPV, focusing on BPV timing and bifurcating SBP variability (SBPV) into two segments (Fig. 1):
1.The hyperacute period, lasting from stroke onset to target SBP attainment (SBPV1), and
2.The acute period, beginning at target SBP attainment and ideally maintained as a sustained plateau (SBPV2)
Fig. 1
SBPV Scenarios with Varying Levels of “Smooth” and “Sustained” Control. The concept of distinct periods of SBPV over time: a ideal “smooth” and “sustained” SBP; b: nonsmooth but sustained BPV; c: smooth but nonsustained BPV; and d neither smooth landing nor sustained control, representing a very suboptimal pattern
There is a precedent for this categorization. Post hoc analyses of INTERACT2 and ATACH-2 only examined SBPV2 to limit bias from study interventions eliciting rapid BP reductions. ATACH-2 investigators did not include BP readings at hours 0–2 after randomization [3], and INTERACT2 BPV analyses excluded BP readings during the first hour after treatment [5]. Conversely, smaller observational studies have included all BP measurements [12, 23].
When managing BPV, this Consortia proposes considering SBPV1 and SBPV2 separately, to address distinct SBPV goals in the hyperacute and acute settings. Consortia proposes that it is ideal to minimize BPV in a smooth (SBPV1) and sustained (SBPV2) manner like an airplane landing (Fig. 1a) or hypothermia protocol after cardiac arrest. Instead, excessive variations in descent and plateau may result in suboptimal outcomes (Fig. 1b–d) and increase the risk of neurologic deterioration hematoma expansion, and/or watershed strokes. However, these concepts require validation in clinical trials.
Practical BPV CalculationMany statistical methods have been crafted to measure BPV, including SD, residual SD, coefficient of variation (CV), successive variation (SV), functional successive variation (FSV), average real variability (ARV), and the difference between the maximum and minimum SBP (max–min) [1,2,3,4, 23,24,25,26]. Although some studies employed one or two of these equations [23] many implemented multiple BPV measures (Table 2) [2,3,4, 27, 28]. This surplus has resulted in no clear standard. To inform these measurements, using an arterial line to continuously monitor SBP will likely provide the most accurate readings and capture sufficient data points, but invasive monitoring is challenging to implement clinically.
Eventually, artificial intelligence (AI) systems may rapidly calculate complex BPV equations in real-time, and translate data into actionable interventions, similar to current AI progress with neuroradiology and neurocardiology [29]. Presently, however, electronic medical records (EMR) are unable to adjust to the dynamic nature of BP over time, typically only recording intermittent, hand-typed BP data [30]. Therefore, we propose using the utilitarian SBP range (max–min) to yield quick and meaningful parameters. This approach, while basic, is supported by retrospective data reporting that SBP ranges are associated with 90-day modified Rankin Scale (mRS) and mortality in both AIS [4, 25] and ICH [3, 5, 6]. Additional testing of BPV measurements and how to incorporate them into clinical practice, especially into EMR with AI, is needed.
Treating Acute Hypertension in StrokeFor AIS, SBP > 185 mm Hg and DBP > 110 mm Hg are IVT relative contraindications, but timely reduction may qualify patients. Patients without IVT receive a “permissive hypertension” strategy (i.e., lowering from > 220 mm Hg to < 220 mm Hg). Although initial SBP control is usually achievable, frequent titration and second/third antihypertensives for “rebound hypertension” are often needed, increasing resource utilization and decreasing efficiencies [31]. After reaching target SBP, minimizing SBPV2 is crucial [18, 31]. Emerging literature shows a relationship between BPV and functional outcomes, highlighting the unmet need for prompt and predictable treatments that minimize SBPV in a “smooth and sustained” manner [32,33,34].
Table 3 summarizes classes of antihypertensives commonly used in hyperacute and acute stroke settings. Bolus dosing, although effective at reducing SBP quickly, carries a risk of increased BPV after administration [34]. Intermediate-to-long-acting antihypertensives may yield smooth reductions in BP, but their longer half-lives preclude timely dose modifications to limit SBPV2 if/when hypotension or overcorrecting occurs [33].
Table 3 Summary of drug classes available for intervention in the acute settingTo limit BPV, ATACH-2 investigators proposed preferential use of a monotherapeutic, short-acting antihypertensive infusion [3]. In a systematic review and meta-analysis, dihydropyridine calcium channel blockers (CCBs) and nonloop diuretics reduced interindividual SBPV more than angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, or beta-blockers [35]. These data identify drug classes that may have consistent effects on SBPV in the hyperacute/acute settings; for example, ultra-short-acting nondihydropyridine CCBs reach prespecified, tight SBP target ranges in 96.9% of patients within 30 min [36]. High-fidelity, high-predictability agents such as the latest-generation CCBs, have been shown to keep SBP within target range (limiting BPV) and limit multiple titrations [36]. Moreover, reducing median time for initial parenteral antihypertensive dose-to-goal (DTG) may result in improved door-to-needle (DTN) thrombolytic times [37] and theoretically less infarcted brain tissue. Future research may focus on prehospital [38] and emergency department DTG and DTN opportunities.
Nitrous vasodilators reach target SBP ranges within 2 min [33, 39] but may significantly increase intracranial pressure, reduce CPP [33, 40] and BP fluctuations are common (only a 69% time within target BP range for ICH) [39]. Nitrous agents therefore are typically avoided for ICH/AIS with cerebral edema, or intracranial mass lesions.
Supporting ATACH-2 investigators’ hypothesis [3] and consistent with AHA/ASA guidelines recommending treatments “that limit BPV and achieve smooth, sustained [BP] control” [7], the Consortia favor shortest-acting intravenous antihypertensive infusions to reach SBP goals while minimizing BPV goals. More research is necessary to determine the optimal antihypertensive regimen in these patients.
Expert Opinion: Proposed BPV TargetsTables 4 and 5 outlines a general approach to defining target SBPV ranges for AIS and ICH, based on intervention status and presenting SBP. These targets represent our expert opinion on SBPV goals and require validation. The scientific rationale for these targets is hypothetical, presumably from vasoplegic arteries that may be prone or sensitive to BPV in the hyperacute phase. For AIS, a reasonable starting point is indentifying SBPV targets by vessel recanalization and IVT/endovascular therapy status (Table 4). For patients with AIS and large-vessel occlusion (LVO) or medium-vessel occlusion (MeVO) who become fully revascularized (TICI 3), there is no flow-dependent deficit. Therefore, fluctuations of < 40 mm Hg during SBPV1 and < 30 mm Hg during SBPV2 may be acceptable. By contrast, in patients with LVO or MeVO and minimal/no revascularization (TICI 0–1), any precipitous SBP drop can exacerbate cerebral ischemia. These patients require particularly cautious SBP lowering and keeping SBPV1 and SBPV2 < 20 mm Hg would be advisable. For patients with partial reperfusion (TICI 2a–2c), the proposed SBPV1 target lies between revascularized and nonrevascularized targets, whereas SBPV2 may need to be < 20 mm Hg.
Table 4 Proposed SBPV targets in AISTable 5 Proposed SBPV targets in ICHFor ICH, the Consortia proposed SBPV targets dependent on presenting SBP (Table 5). For patients with SBP > 220 mm Hg, tight SBPV1 and SBPV2 goals are desirable because these extremely hypertensive individuals may be at greatest risk of ischemia with major BP drops. For patients with SBP 180–220 mm Hg, we suggest an SBPV1 goal of < 30 mm Hg and a tighter goal in SBPV2. For patients with SBP 140–180 mm Hg, a relatively loose SBPV1 of < 40 mm Hg and SBPV2 of < 20 mm Hg may be permissible. Lastly, normotensive patients may tolerate wider SBPV ranges in both phases.
Comments (0)