An Exploratory Analysis of Chemical and Mechanical VTE Prophylaxis in Patients with High Rebleeding Risk Traumatic Brain Injury
Background
There is little research on venous thromboembolism (VTE) prophylaxis (PPX) timing of the higher rebleeding risk groups based on size and type of traumatic brain injury (TBI) due to exclusion from previous observational studies, which prohibits the facilitation of an evidence-based strategy. We aim to determine the effect of VTE PPX timing on the high rebleeding risk TBI population based on the modified Berne Norwood Criteria.
Methods
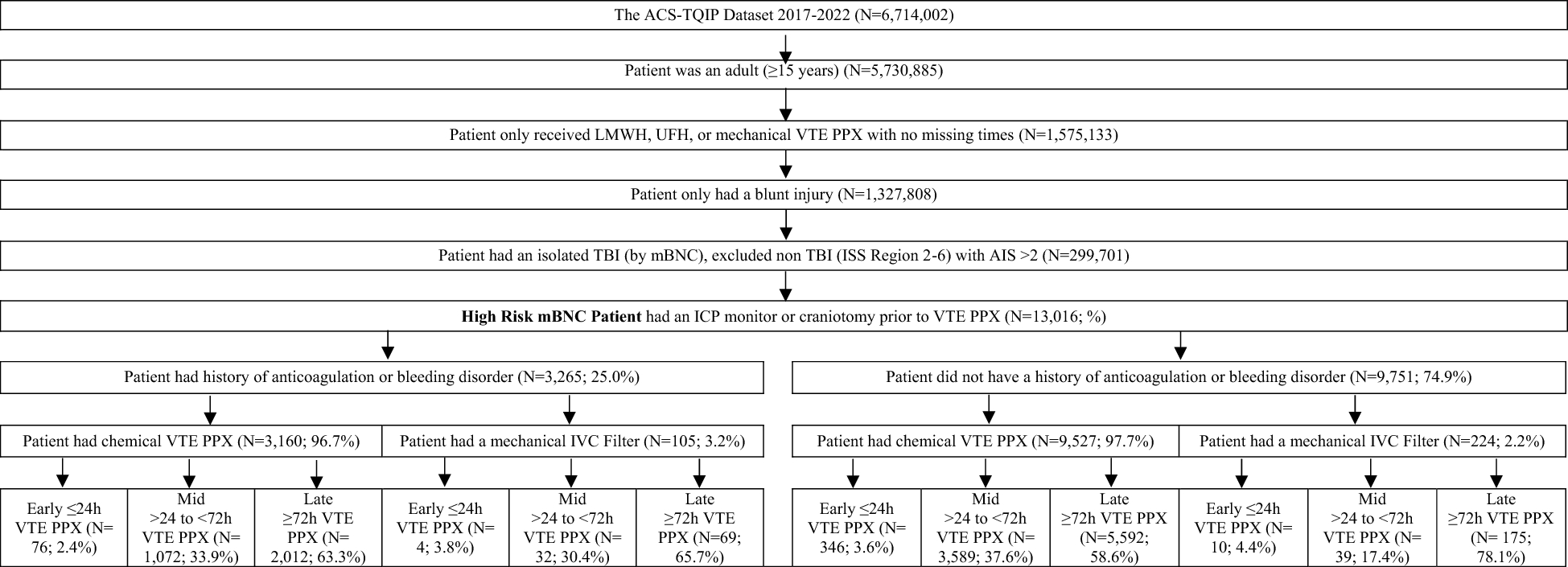
This retrospective cohort study used the American College of Surgeons Trauma Quality Program Participant Use File from 2017 to 2022. The study population consisted of adult patients who received chemical or mechanical PPX with no missing times and had a blunt high rebleeding risk TBI stratified by a comorbid history of anticoagulation or bleeding disorder with excluded polytrauma. There was a total of 12 exposure groups based on VTE PPX timing with the outcomes of interest being intensive care unit (ICU) stay, ventilation days, and mortality.
Results
A total of 13,016 patients were included in the exploratory analysis. Early initiation of chemical VTE PPX (within ≤ 24 h) was associated with a reduced likelihood of prolonged ICU stay and ventilation days, regardless of prior anticoagulation use or bleeding disorder. In contrast, inferior vena cava filter placement within the > 24-h to < 72-h window was associated with increased ICU and ventilation duration.
Conclusions
This study highlights the benefits of initiating chemical VTE PPX within 24 h for patients wih high rebleeding risk TBI, demonstrating significant reductions in ICU stays and ventilation days without an increase in mortality rates. Additionally, although inferior vena cava filters are associated with longer ICU stays and increased ventilation days, this may reflect the greater severity and potential mortality risk of the conditions being treated.

Comments (0)