Study Design and Participants
The i-DEF (ClinicalTrials.gov identifier: NCT02175225) trial was a multicenter randomized, placebo-controlled phase 2 clinical trial conducted across 40 centers in the United States and Canada. The trial investigated the iron chelator deferoxamine mesylate as a treatment option against secondary brain injury after ICH, in which iron from hemolyzed blood has been implicated. Its methodology, including details about data collection and imaging analysis, is described elsewhere [7, 8]. In short, i-DEF participants had primary supratentorial ICH and were randomized to receive study drug infusions for three consecutive days, starting within 24 h of ICH onset. Patients with known severe anemia (Hb level < 7 g/dL or requiring blood transfusions), coagulopathy (prolonged activated partial thromboplastin time or elevated international normalized ratio on presentation, or use of direct oral anticoagulants or low-molecular-weight heparin), planned hematoma evacuation, and infratentorial or secondary ICH were excluded from participation. Screening in the i-DEF trial included standardized laboratory assessments, including hematology, done locally at each site as part of routine care. Head computed tomography (CT) was obtained at screening (baseline scan) and within 24 h of completion of the last infusion (i.e., within 72–96 h from ICH onset; follow-up scan). CT scans were sent to a core imaging laboratory (Beth Israel Deaconess Medical Center, Boston, MA). Imaging evaluations were done by experienced blinded raters using an imaging analysis software (Analyze 11.0; AnalyzeDirect, Overland Park, KS). Volumetric assessments of intracerebral hematoma and PHE were done on CT scans using a validated Hounsfield-unit-threshold-based, semiautomated segmentation approach with manual correction, as described previously and in Supplementary Fig. 1 [7, 8].
In this exploratory post hoc analysis focusing on the association of Hb with PHE, we included all i-DEF participants with available laboratory and imaging data. We excluded those with emergent surgical treatment (craniectomy/hematoma evacuation) because this may impact PHE growth.
Exposures and Outcomes
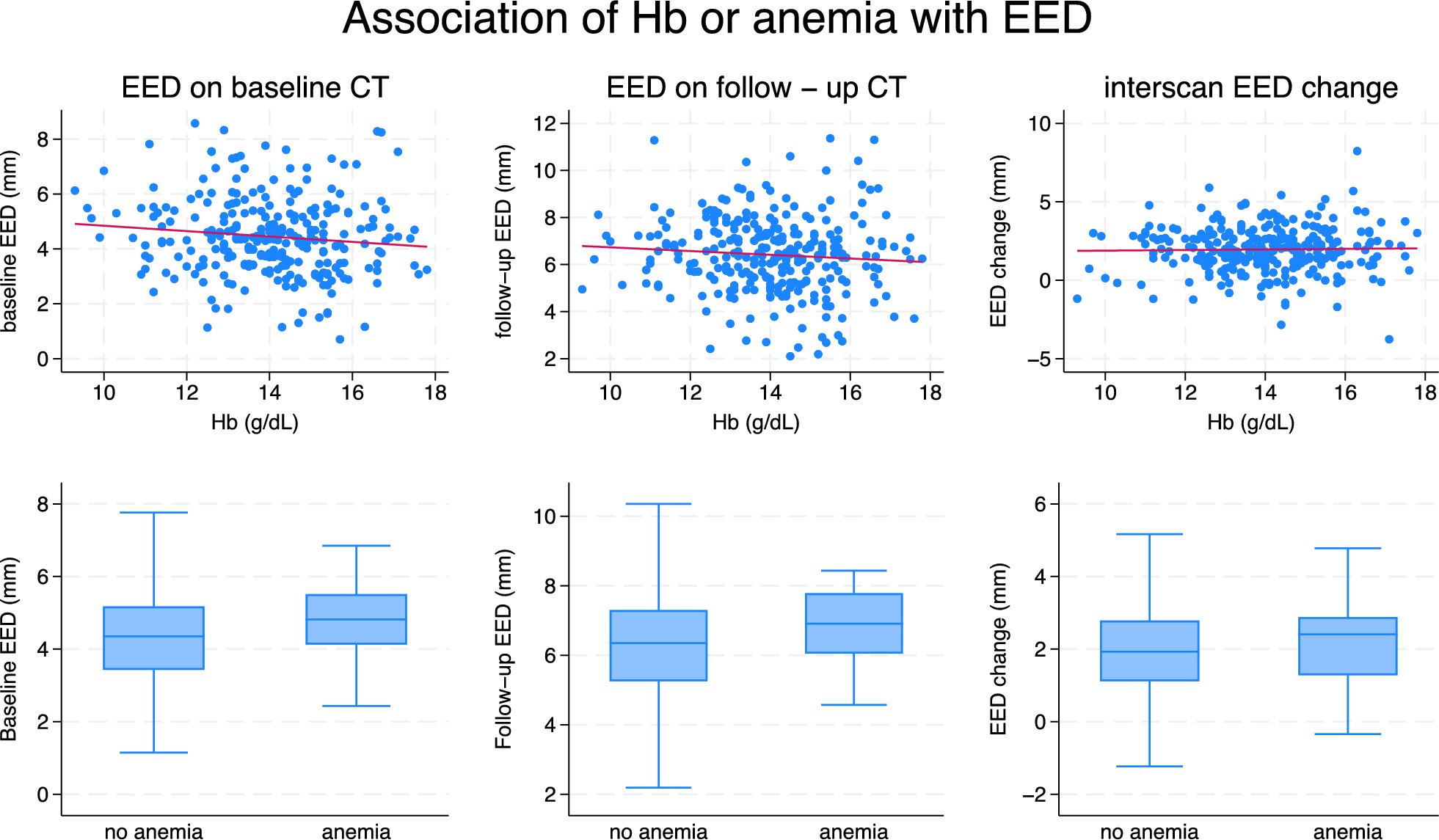
The main exposures were Hb (as a continuous variable) and anemia (as a dichotomous one) at screening. The latter was defined as Hb level < 12 g/dL for women and < 13 g/dL for men as per standard World Health Organization definitions.
The main outcome was PHE assessed as edema extension distance (EED; as continuous variable, expressed in mm, defined as the difference between the radius of a sphere equal to the combined ICH and PHE volume and the radius of a sphere equal to the ICH volume alone) [9]. We assessed EED as a single measurement on the baseline and follow-up scans, and as its interscan change. We chose EED as the main outcome because it has been shown to be independent of hematoma volume and more advantageous over other metrics to study the effects of exposures on PHE [9, 10]. In ancillary analyses, we similarly investigated absolute PHE volume (aPHE) and relative PHE (rPHE; defined as the ratio of aPHE to ICH volume), both as continuous outcomes. Although only rPHE was investigated in the main i-DEF trial, subsequent analyses have reported on aPHE and EED in the i-DEF data set before [7, 8].
Statistical Analysis
We present all data using descriptive statistics. We compared categorical and continuous variables using the χ2 test or Fisher’s exact test and the Mann–Whitney U-test or t-test, respectively, as appropriate. We assessed the relationship between Hb and PHE measures using Spearman correlation. We further investigated the association of Hb or anemia with PHE measures in (1) unadjusted, (2) partially adjusted, and (3) fully adjusted linear regression models. Partially adjusted models included as covariates known determinants of Hb (sex, age, and race) [11] and the most essential potential determinants of baseline PHE [12] (baseline ICH volume and time from ICH onset to baseline scan) or its progression (interscan time, use of hyperosmolar therapy [hypertonic saline and/or mannitol], and actual i-DEF treatment received [deferoxamine or placebo]). Fully adjusted models additionally included the following potential outcome modifiers: serum glucose level, ICH location (lobar, thalamic, or deep nonthalamic), ICH score (comprising Glasgow Coma Scale score, age, ICH volume, intraventricular hemorrhage, and infratentorial ICH location), previous use of antithrombotics (antiplatelets or anticoagulants), and external ventricular drain placement before follow-up scan. We chose to include external ventricular drain placement because this may capture several relevant aspects worth accounting for, including its potential treatment effects and a broader reflection of morbidity and ICH severity [13, 14]. There were no missing values in any of these covariates. Because of skewed distributions, we log-transformed ICH volume, aPHE, and rPHE for regression analyses. We report correlation coefficients (ρ) and model-based (β coefficient) estimates with 95% confidence intervals (CIs) as measures of association. For log-transformed PHE measures, we report back-transformed estimates (βmult), which represent multiplicative effects on the geometric mean of the PHE measure. We present p values for all tests but refrain from defining significance thresholds or from correcting for multiple testing given the exploratory nature of the study. We performed all analyses using STATA 18.0 (StataCorp LLC, College Station, TX). We conducted this study in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement.

Comments (0)