
Remember me









Adequate bowel preparation is essential for a high-quality colonoscopy, but 10%–25% of colonoscopy failures are a result of inadequate bowel preparation (1), which is associated with prolonged procedural time, cecal intubation failure, and missed lesions. Constipation has been identified as 1 of the independent risk factors for inadequate bowel preparation (2).
Constipation is a common gastrointestinal disorder that affects 12%–17% of the world's population (3), compromising their quality of life. Approximately 11.9%–17.5% of patients undergoing colonoscopy are constipated (4,5). Many guidelines recommend the four-liter (4L) PEG scheme, a low-residue diet, or gastrointestinal kinetic drugs before endoscopy to improve bowel preparation in patients with risk factors such as constipation (5,6). However, patient satisfaction and quality of bowel preparation are still not optimal (7). It is necessary to find other effective methods to increase the efficiency of bowel preparation.
Polyethylene glycol electrolytes (PEG) are widely used as bowel cleansers during colonoscopy (8), but the PEG regimens alone remain unsatisfactory in patients with chronic constipation (CC) because of dose intolerance. A study showed that compared with the 4L-PEG regimen, 2L-PEG plus bisacodyl improved colonic mucosa visualization, patient acceptance, and compliance in patients with CC, but did not increase the bowel cleansing efficiency (9). Another study showed that PEG combined with tegaserod during colonoscopy did not improve the quality of colonic preparation, patient tolerance, or adverse side effects (10). Therefore, more attempts should be made to improve the quality of bowel preparation.
Linaclotide is a guanine cyclase C agonist that promotes intestinal fluid secretion, accelerates colon transport, and alleviates visceral pain by the intracellular or extracellular cyclic guanosine, and is used for the treatment of CC and irritable bowel syndrome with constipation, with a favorable safety profile and few adverse effects in long-term therapy (11). A previous study showed that single-dose linaclotide before capsule endoscopy was equally effective compared with PEG in terms of visualization and transit time (12). Recently, a study found that the regimen of 1L-PEG and linaclotide was not inferior to 2L-PEG in terms of colon cleansing, with better tolerability and higher willingness to repeat the bowel preparation in a low-risk population (13). No studies have been conducted to explore the efficacy of bowel preparation by PEG combined with linaclotide in patients with CC.
METHODS PatientsThis was an endoscopist-blinded, randomized, controlled, and multicenter study of patients with constipation who underwent colonoscopy between July 2021 and December 2022 at 7 hospitals in Northwest China. The study was approved by the Ethics Committee of the Second Affiliated Hospital of Xi'an Jiao Tong University, and written informed consent was obtained from all participants.
The enrolled patients were aged ≥18 years, met the Rome Ⅳ criteria of functional constipation, and willingly underwent colonoscopy. Specifically, the Rome IV criterion was the presence of ≥ 2 of the following: (i) straining for >25% of defecations, (ii) lumpy or hard stools (form 1 or 2 on the Bristol Stool Form Scale) for >25% of defecations, (iii) sensation of incomplete evacuation for >25% of defecations, (iv) sensation of anorectal obstruction/blockage for >25% of defecations, (v) manual maneuvers to facilitate defecation for >25% of defecations, or (f) <3 spontaneous bowel movements per week (14). The patients had to have symptoms for at least 6 months before the diagnosis by doctors.
Exclusion criteria: (i) age <18 years; (ii) severe chronic renal failure, severe congestive heart failure, or liver dysfunction; (iii) uncontrolled hypertension, diabetes, intestinal obstruction, intestinal perforation or electrolyte disorders, inflammatory intestinal disease, or other organic gastrointestinal diseases; (iv) neurologic, endocrine, or metabolic disorders; (v) treatment with all drugs affecting gastrointestinal function within the past 2 weeks; (vi) history of colorectal surgery; (vii) dysphagia; (viii) compromised swallowing reflex or mental status; (ix) consciousness disorders or examination intolerance; (x) pregnancy or lactation; (xii) allergy to any drug component; (xii) suspected history of alcohol or substance abuse; (xiii) recent participation in a clinical trial; and (xiv) lack of informed consent.
Randomization and blindingEligible patients were randomly divided into 4 groups (1:1:1:1) based on a computer-generated list of randomized numbers at the time of the appointment for colonoscopy: the 4L-PEG group, the 4L-PEG+1d-Lin group, the 3L-PEG+1d-Lin group, and the 3L-PEG+3d-Lin group. All experienced endoscopists (>2,000 colonoscopies) trained in the BBPS scoring system were blinded to the patient assignment before and during the procedure.
Bowel preparationAll patients were informed and educated about the procedure by the doctors, and they were instructed regarding the exact colon preparation procedure, the importance of bowel preparation for CC, and the side effects of the agents used. Then, the patients signed the consent form, and they were prescribed polyethylene glycol electrolyte powder (PEG, 12A + 12B; WanHe Pharmaceutical Co, Shenzhen, China) or linaclotide (290 μg/capsule, AstraZeneca) for bowel preparation. The baseline demographic and clinical characteristics of the patients were recorded.
All patients followed a low-fiber diet on both the third and second day before the procedure, followed by a clear fluid diet the day before and the morning of the colonoscopy. Patients with 1-day linaclotide were given at 6:00 am on the day of colonoscopy; patients with 3-day linaclotide were given at 6:00 am on the day of colonoscopy and 2 days before colonoscopy. They were instructed to drink 1 or 2L of PEG at 8:00 pm the day before their colonoscopy and to drink the remaining 2L-PEG at 8:00 am on the day of colonoscopy. All colonoscopies were performed in the afternoon (between 1:00 and 3:00 pm). Endoscopists used a foot pedal for lavage.
Data collection and colonoscopyBefore the colonoscopy, patients were interviewed by investigators not involved in the endoscopic procedure. Patient demographic data (including age, sex, marital status, and educational background), use of purgatives, start time of bowel preparation, side effects (recalled details of abdominal fullness, abdominal pain, nausea, and vomiting after bowel preparation), the time of first defecation (duration of the time from taking the PEG to the first bowel movement) and defecation frequency (the number of bowel movements after drinking PEG), sleep quality, and willingness to repeat the bowel preparation were recorded. After the examinations, the investigators also recorded the quality of the bowel preparation, cecal intubation time, withdrawal time excluding the time required for polypectomy or biopsy, and colonoscopic findings, including the polyp detection rate and adenoma detection rate for all patients.
Outcome measuresAfter the colonoscopy, the effectiveness of bowel cleansing was assessed according to the Boston Bowel Preparation Scale (BBPS) (15). The primary outcome was adequate bowel preparation, defined as a total BBPS score ≥6 and a score ≥2 for each segment (16). The secondary outcomes were the polyp detection rate, adenoma detection rate, adverse events, willingness to repeat the bowel preparation, cecal intubation time, and withdrawal time.
Calculation of sample sizeIn the study protocol, the sample size calculation was performed with an alpha of 0.05 and a power of 0.8, assuming a 10% difference in the rate of colonic cleansing and a 20% dropout rate (17,18). The rate of adequate bowel preparation in our endoscopic center was 62.8% among patients with functional constipation (19). Therefore, we calculated that at least 406 patients were needed for the study by using Power Analysis and Sample Size 11.
Statistical analysisStatistical analyses were performed for the per-protocol analyses. The intention-to-treat analyses included all randomized participants who provided written informed consent, regardless of whether the participants successfully completed the colonoscopy. The per-protocol analyses included all study participants who successfully completed the colonoscopy according to the study protocol.
Numeric variables were presented as the mean ± SD and analyzed by the T-test or Mann‒Whitney test. One-way analysis of variance with the least significant difference post hoc test was used to compare mean values. The enumeration data were described as frequencies or rates and analyzed by the χ2 test or Fisher exact test. SPSS software (version 22.0; IBM) was used to analyze the collected data, and P values < 0.05 were considered statistically significant.
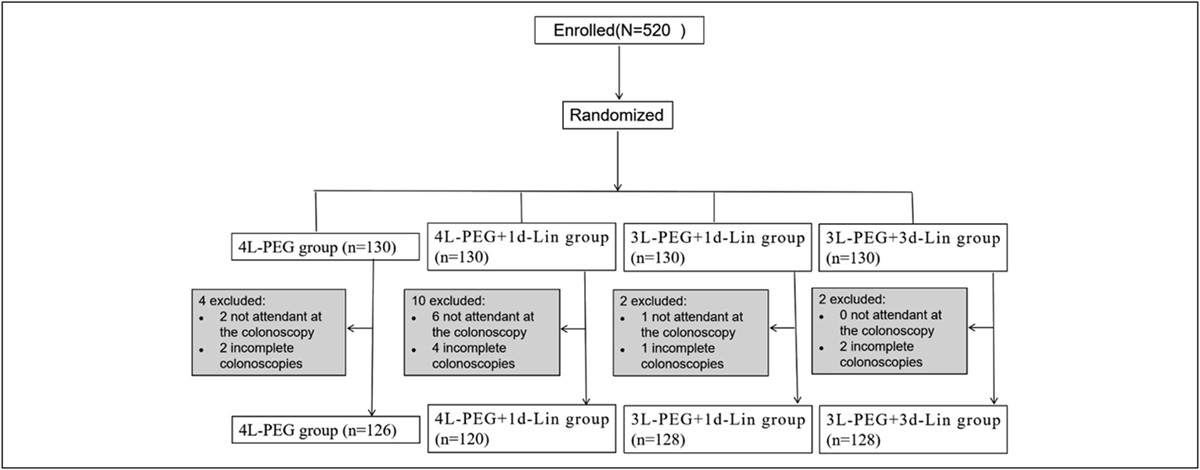
RESULTS Patient characteristicsA total of 502 consecutive patients with CC who met the inclusion criteria and were successfully enrolled in the study were randomly assigned to 4 different groups: the 4L-PEG group (n = 126), the 4L-PEG+1d-Lin group (n = 120), the 3L-PEG+1d-Lin group (n = 128), and the 3L-PEG+3d-Lin group (n = 128) (Figure 1). At baseline, the 4 groups did not significantly differ in age, sex, life conditions, grade of constipation, or the duration of CC, although they did in body mass index (Table 1).
 Figure 1.:
Figure 1.: Study flow chart. BBPS, Boston Bowel Preparation Scale; PEG, polyethylene glycol electrolyte powder; lin, linaclotide.
Table 1. - Baseline patient characteristics 4L-PEG group, N = 126 4L-PEG+1d-Lin, N = 120 3L-PEG+1d-Lin, N = 128 3L-PEG+3d-Lin, N = 128 P value Sex, n (%) Male 22 (17.5%) 28 (23.3%) 20 (15.6%) 28 (21.9%) 0.373 Age, mean ± SD 49.98 ± 10.42 48.40 ± 11.59 51.22 ± 6.48 49.03 ± 10.09 0.735 BMI, mean ± SD 23.51 ± 3.46 23.12 ± 3.25 23.11 ± 2.68 22.30 ± 3.15 0.048 Smoking 21 (16.7%) 20 (16.7%) 16 (12.5%) 28 (21.9%) 0.259 Alcohol drinking 21 (16.7%) 28 (23.3%) 28 (21.9%) 28 (21.9%) 0.583 Grade of education, n (%) 0.163 Elementary or below 11 (8.7%) 16 (13.3%) 24 (18.8%) 24 (18.8%) Junior high school 31 (24.6%) 28 (23.3%) 36 (28.1%) 28 (21.9%) High school or above 84 (66.7%) 76 (63.3%) 68 (53.1%) 76 (59.4%) Long-term residence, n (%) 0.283 Town 109 (86.5%) 112 (93.3%) 116 (90.6%) 112 (87.5%) Country 17 (13.5%) 8 (6.7%) 12 (9.4%) 16 (12.5%) Degree of constipation,a n (%) Mild 65 (51.6%) 60 (50.0%) 64 (50.0%) 64 (50.0%) 0.169 Moderate 28 (22.2%) 36 (30.0%) 44 (34.4%) 44 (34.4%) Severe 33 (26.2%) 24 (20.0%) 20 (15.6%) 20 (15.6%) Drinking in the morning 93 (73.8%) 92 (76.6%) 88 (68.8%) 88 (68.8%) 0.42 Degree of straining ≥25% 55 (43.7%) 64 (53.3%) 76 (59.4%) 64 (50.0%) 0.09 No. of bowel movements per wk ≥3 37 (29.4%) 36 (30.0%) 56 (43.8%) 36 (28.1%) 0.60BMI, body mass index.
aDegree of constipation: According to the severity of symptoms and impact on daily life, constipation can be divided into 3 degrees: mild symptoms are mild and do not affect patient's life, and patients can rebuild normal defecation through overall treatment and short-term medication. Severe—symptoms are severe and lasting and greatly impact patient's work and life. Medications are needed, cannot be interrupted, or may be even ineffective. Moderate fall in between mild and severe.
The quality of bowel preparation was assessed using the BBPS. Compared with the 4L-PEG group, the rate of adequate preparation was significantly higher in the 3L-PEG+3d-Lin group (84.4% vs 60.3%, P < 0.001) and the 4L-PEG+1d-Lin group (80.0% vs 60.3%, P < 0.001) (Figure 2). There were no significant differences in the rate of adequate preparation between the 3L-PEG+3d-Lin group and the 4L-PEG+1d-Lin group (84.4% vs 80.0%, P > 0.05) or between the 4L-PEG group and the 3L-PEG+1d-Lin group (60.3% vs 62.50%, P > 0.05). Similarly, the total BBPS score in the 3L-PEG+3d-Lin group or the 4L-PEG+1d-Lin group was significantly higher than that in the 3L-PEG +1d-Lin group (7.03 ± 1.24 vs 6.31 ± 1.77, P = 0.003; 6.90 ± 1.28 vs 6.31 ± 1.77, P = 0.003) or the 4L-PEG group (7.03 ± 1.24 vs 6.00 ± 1.61, P < 0.001; 6.90 ± 1.28 vs 6.00 ± 1.61, P < 0.001). In the right colon, the BBPS scores in the 3L-PEG+3d-Lin group (2.19 ± 0.53) and the 4L-PEG+1d-Lin group (2.10 ± 0.54) were higher than those in the 4L-PEG group (1.78 ± 0.67) (P < 0.001; P < 0.001) and the 3L-PEG+1d-Lin group (1.78 ± 0.86) (P = 0.007; P < 0.001) (Table 2).
 Figure 2.:
Figure 2.: The rate of adequate bowel preparation. Adequate bowel preparation: The total BBPS score ≥6 and all segment scores ≥2. *vs the 4L-PEG group, P < 0.05.
Table 2. - Comparison of the quality of bowel preparation 4L-PEG group, N = 126 4L-PEG+1d-Lin, N = 120 3L-PEG+1d-Lin, N = 128 3L-PEG+3d-Lin, N = 128 P value Right side of colon (mean ± SD) 1.78 ± 0.67 2.10 ± 0.54 1.78 ± 0.86 2.19 ± 0.53 <0.001 Mid-colon (mean ± SD) 2.23 ± 0.67 2.40 ± 0.56 2.37 ± 0.70 2.50 ± 0.50 0.021 Rectosigmoid colon (mean ± SD) 1.99 ± 0.66 2.37 ± 0.66 2.19 ± 0.64 2.34 ± 0.74 <0.001 Total score (mean ± SD) 6.00 ± 1.61 6.90 ± 1.28 6.31 ± 1.77 7.03 ± 1.24 <0.001 Cecal intubation time (min, mean ± SD) 6.87 ± 2.54 8.07 ± 5.34 8.91 ± 4.27 6.98 ± 3.52 <0.001 Withdrawal time (min, mean ± SD) 8.75 ± 4.27 7.81 ± 3.98 7.78 ± 2.77 7.65 ± 2.24 0.268 Total examination time (min, mean ± SD) 15.37 ± 5.42 15.79 ± 7.61 16.69 ± 5.52 14.63 ± 4.49 0.003 The first time of defecation (h, mean ± SD) 1.28 ± 0.77 1.25 ± 1.33 1.31 ± 1.57 1.18 ± 0.95 0.001 Defecating frequency 9.02 ± 1.99 10.53 ± 2.75 10.25 ± 3.84 10.09 ± 3.15 0.001 Preparation-to-colonoscopy interval (h, mean ± SD) 4.72 ± 0.69 4.86 ± 1.07 4.78 ± 0.91 4.78 ± 0.85 0.674 Polyp detection rate, n (%) 27 (21.4) 39 (32.5) 34 (26.6) 41 (32.0) 0.169 Adenoma detection rate, n (%) 21 (16.7) 30 (25.0) 26 (20.3) 32 (25.0) 0.308The polyp detection rate and adenoma detection rate were higher in the 3L-PEG+3d-Lin group and the 4L-PEG+1d-Lin group than those in the 4L-PEG group (Table 2), but the differences were not statistically significant (P > 0.05). The total examination time and the first time of defecation were lowest in the 3L-PEG+3d-Lin group (P < 0.001). The defecation frequency after bowel cleaning in the 4L-PEG group was lower than that in the other groups (P = 0.001). There were no statistically significant differences among the groups in the withdrawal time, defecation frequency of the first time, the second time of defecation, and preparation-to-colonoscopy interval (Table 2).
Patient adverse events and tolerabilityIn total, 355 (70.7%) patients presented with mild adverse events that were mostly associated with bowel preparation, including slight abdominal fullness, abdominal pain, nausea, and vomiting, without the most frequent treatment-emergent adverse events (Table 3). The percentage of complications was significantly highest in the 4L-PEG group among all groups (81.8% vs 66.7%, 58.6%, 75.0%, P = 0.001), especially regarding abdominal bloating and pain (Table 3). The rates of willingness to repeat the colonoscopy and poor sleep before the colonoscopy were not different between any groups (P = 0.579, P = 0.075).
Table 3. - The rate of patient adverse events and tolerance 4L-PEG group, N = 126 4L-PEG+ 1d-Lin, N = 120 3L-PEG+ 1d-Lin, N = 128 3L-PEG+ 3d-Lin, N = 128 P value Adverse events, n (%) 103 (81.8) 80 (66.7) 75 (58.6) 96 (75.0) 0.001 Nausea, n (%) 38 (30.2) 20 (16.7) 36 (28.1) 44 (34.4) Vomiting, n (%) 5 (4.0) 4 (3.3) 4 (3.1) 4 (3.1) Abdominal pain, n (%) 11 (8.7) 12 (10.0) 4 (3.1) 0 (0) Bloating, n (%) 49 (38.9) 44 (36.7) 31 (24.2) 48 (37.5) Willingness to repeat the colonoscopy, n (%) 56(44.4) 60 (50.0) 68 (53.1) 64 (50.0) 0.579 Poor sleep, n (%) 12 (9.5) 8 (6.7) 4 (3.1) 4 (3.1) 0.075Adequate bowel preparation is essential for diagnosing and treating intestinal diseases, especially for patients with risk factors, such as CC. We found that compared with 4L-PEG, 4L-PEG with linaclotide for 1 day or 3L-PEG with linaclotide for 3 days before colonoscopy provided a more significant benefit in bowel preparation quality among patients with CC. The quality of bowel preparation was similar between the 4L-PEG+1d-Lin group and the 3L-PEG+3d-Lin group. Few multicenter studies have evaluated PEG in combination with linaclotide to improve bowel preparation in patients with CC.
The BBPS is a valid and reliable instrument for rating the quality of bowel preparation during colonoscopy (15). One study showed that the PEG combined with lubiprostone (LB, 24 µg) could enhance the rate of adequate bowel preparation, rather than affecting the mean total and segment-specific BBPS scores (20). Conversely, another study showed that the PEG combined with mosapride could elevate the total BBPS score with better bowel preparation efficacy and lower adverse events, as opposed to affecting the rate of adequate bowel preparation (BBPS ≥6) (21). In our study, the rates of adequate bowel preparation and the total BBPS score were significantly higher in the 4L-PEG+1d-Lin group compared with the 4L-PEG group, as well as the 3L-PEG+3d-Lin group compared with the 3L-PEG+1d-Lin group. Linaclotide, as an adjunctive agent to PEG, leads to better quality cleansing. Because PEG functions as an osmotic laxative and linaclotide acts as a guanine cyclase C receptor agonist, we hypothesized that the drug combination may promote their individual effects on bowel cleansing through 2 different mechanisms.
In addition, adenoma detection rate (ADR) and polyp detection rate are also important indicators of endoscopy quality (15). One study found that the higher the segmental BBPS was, the higher the ADR and advanced ADR showed (22). Consistent with our findings, the 3L-PEG+3d-Lin group or the 4L-PEG+1d-Lin group had higher BBPS scores and exhibited higher rates of polyp and adenoma detection, compared with the 3L-PEG+1d-Lin group (57.0% vs 46.9%) or the 4L-PEG group (57.7% vs 37.1%), respectively, with no statistical significance. Those results also indicated that the combination of PEG and linaclotide before colonoscopy enhanced the efficacy of bowel preparation.
Patient compliance and tolerability are also closely connected with high-quality bowel preparation and are essential for successful colonoscopies (23). Many clinical guidelines recommend the use of 4L-PEG solution in patients with CC (5,6,24), but some patients have poor compliance and tolerance of this solution because of the large amounts of liquid that must be swallowed. Low-volume bowel preparations have improved patient tolerability compared with large-volume PEG preparations (25,26). In a recent study, high-volume PEG (2L + 2L) yielded clinically similar results compared with low-volume PEG (1L + 1L) plus bisacodyl (15 mg); however, patients' willingness to repeat and their tolerability were superior in the low-volume group (27). For patients in the difficult-to-cleanse population, the PEG 2+2L + bisacodyl was more efficacious in bowel cleansing than the PEG 4+2L + bisacodyl (28). These results showed that the high-volume PEG alone is not the optimal strategy for patients with risk factors for inadequate bowel preparation. In addition, bisacodyl, a stimulant laxative, was more likely to lead to adverse events than linaclotide in treatment of constipation (29,30). In our study, linaclotide is approved by the US Food and Drug Administration for the treatment of irritable bowel syndrome with constipation and chronic idiopathic constipation (31). In numerous clinical trials, the efficacy and safety profiles of linaclotide have been demonstrated, with minimal systemic absorption, high safety, and few clinical complications (6,24,32). A study (33) showed that the efficacy of 2L-PEG combined with 290-μg linaclotide was similar to that of 4L-PEG and was superior to that of 2L-PEG for precolonoscopy preparation, but patients in their high-volume 4L-PEG group had the highest rates of complications, with symptoms of nausea, vomiting, bloating, and abdominal pain. In our study, the rate of adverse events was higher in the 4L-PEG group than in the 4L-PEG + 1d-Lin group, especially in nausea. Compared with the 3L-PEG + 1d-Lin group, the rate of adverse effects was higher in the 3L-PEG + 3d-Lin group with better quality of bowel preparation, but those were mild without serious side effects. Besides, we found the total rate of adverse events in the 4L-PEG group was the highest, whereas the rate of the willingness to repeat colonoscopy was the lowest, although there were no differences among groups. In summary, bowel cleansing before colonoscopy with linaclotide is effective and safe in patients with constipation.
CC is an independent risk factor for inadequate bowel preparation for colonoscopy (4,5), which can be ameliorated by promoting defecation function. One study (19) suggested that the Bristol Stool Form Scale 1, starting-to-defecation interval ≥4 hours, and no or mild pain during defecation were independent high-risk factors for inadequate bowel preparation in constipated patients, and these factors could be improved by different targeted solutions (34,35). Other studies have shown that enhanced education with detailed information on bowel preparation by telephone (36), WeChat (37), or short message service (38) on the day before colonoscopy could improve patient compliance and bowel preparation quality. Identifying risk factors for poor bowel preparation and developing interventions can help reduce the incidence of inadequate bowel preparation. In this study, there was a higher quality of intestinal clearance in the 4L-PEG+1d-Lin group or the 3L-PEG+3d-Lin group than in the 4L-PEG group or the 3L-PEG+1d-Lin group, which might be due to the therapeutic function of linaclotide for constipation.
Adequacy of bowel cleansing also mainly depends on the timing of colonoscopy. In our study, all colonoscopies were scheduled for the afternoon. Previous research has indicated the rates of inadequate bowel preparation and incompletion were higher in afternoon colonoscopies compared with morning colonoscopies (39). Subsequently, a meta-analysis showed no significant difference in colonoscopy quality between morning and afternoon colonoscopies, when a half-day shift prevented endoscopist fatigue, and spilt-dose bowel preparation improved bowel preparation for colonoscopies scheduled in the afternoon (40). Recent studies have demonstrated that a split-dose PEG regimen was provided for morning colonoscopies, and a same-day PEG regimen was used for afternoon colonoscopies (41,42). In our study, linaclotide was taken 2 hours before taking the last 2L-PEG on the morning of the colonoscopy, coupled with the guideline recommendation of a 4- to 6-hour preparation-to-colonoscopy interval for better cleansing (43), thereby promoting the scheduling of all colonoscopies in the afternoon. Consequently, improving cleansing protocols, especially for the timing of linaclotide administration, may be beneficial in enhancing the quality of bowel preparation.
In addition, a good regimen for bowel preparation also should be tailored to the individual facts and wishes of the patients. In our study, the cleansing effects of the 4L-PEG+1d-Lin group and the 3L-PEG+3d-Lin group were similar. For patients with poor compliance to long-term bowel preparation or patients with urgent preparation time who need to complete a colonoscopy as soon as possible, 4L-PEG+1d-Lin can be chosen. For patients with good compliance, plenty of time, and intolerance to the use of large amounts of fluid, 3L-PEG+3d-Lin can be considered.
There are also some limitations to our study. First, although this was a multicenter study, the patients were mainly from northwest China, which does not represent other areas because of differences in diet, environment, and genetics. Second, some information about the participants and bowel preparation was self-reported, so recall error and response bias were unavoidable. Finally, there are no data provided for the indication of colonoscopy, which limits applicability of this study into the daily clinical practice.
In conclusion, the efficacy of 3L-PEG combined with 290 μg (3 days) of linaclotide was similar to that of 4L-PEG combined with 290 μg (1 day) of linaclotide and was superior to that of 4L-PEG for colonoscopy preparation in patients with CC.
CONFLICTS OF INTERESTGuarantor of the article: Fei Dai, MD, PhD.
Specific author contributions: F.D.: developed the study concept and design. X.H.W., Q.Y., J.P.H., K.Z., J.H.W., S.H.W., X.J.Q., X.Q.M., F.W., and S.H.: designed and trained colonoscopy. X.R.L., Y.H.S., H.G.H., and Y.D.C.: acquired the data. L.L.W., Y.Z., J.Y.L., L.F.L., and Y.R.: analyzed the data. L.L.W. and F.D.: wrote the first draft of the manuscript. F.D. and X.H.W.: made critical revisions to the paper.
Financial support: The study was funded by National Natural Science Foundation of China (NO. 81770540) and the Key Research and Development Projects of Shaanxi Province (S2023-YF-YBSF-1670).
Potential competing interests: None to report.
IRB approval statement: This study was approved by the Ethics Committee of the Second Affiliated Hospital of Xi'an Jiao Tong University (Scientific Research No.2021-030).
This study was registered at ClinicalTrials.gov (NCT05137145).
Study Highlights
WHAT IS KNOWN ✓ Current bowel preparation regimens for patients with chronic constipation remain unsatisfactory in bowel cleansing effects and produce uncomfortable side effects. ✓ There were rare randomized clinical trials investigating PEG combined with linaclotide for colonoscopy in patients with chronic constipation. WHAT IS NEW HERE ✓ Linaclotide combined with PEG before colonoscopy was an effective method for bowel cleansing in patients with chronic constipation. ✓ The present bowel preparation regimens improved bowel preparation and caused few severe adverse reactions. REFERENCES 1. Chokshi RV, Hovis CE, Hollander T, et al. Prevalence of missed adenomas in patients with inadequate bowel preparation on screening colonoscopy. Gastrointest Endosc 2012;75(6):1197–203. 2. Paik N, Kim ER, Kim TJ, et al. Usefulness of personal bowel habits as a predictive factor for inadequate bowel preparation for colonoscopy: A prospective questionnaire-based observational study. Gut and liver 2019;13(2):169–75. 3. Suares NC, Ford AC. Prevalence of, and risk factors for, chronic idiopathic constipation in the community: Systematic review and meta-analysis. Am J Gastroenterol 2011;106(9):1582–92; quiz 1, 92. 4. Dik VK, Moons LM, Hüyük M, et al. Predicting inadequate bowel preparation for colonoscopy in participants receiving split-dose bowel preparation: Development and validation of a prediction score. Gastrointest Endosc 2015;81(3):665–72. 5. Gimeno-García AZ, Baute JL, Hernandez G, et al. Risk factors for inadequate bowel preparation: A validated predictive score. Endoscopy 2017;49(6):536–43. 6. Johnson DA, Barkun AN, Cohen LB, et al. Optimizing adequacy of bowel cleansing for colonoscopy: Recommendations from the US multi-society task force on colorectal cancer. Am J Gastroenterol 2014;109(10):1528–45. 7. Sweetser S, Baron TH. Optimizing bowel cleansing for colonoscopy. Mayo Clinic Proc 2015;90(4):520–6. 8. Ichijima R, Suzuki S, Esaki M, et al. Efficacy of macrogol 4000 plus electrolytes in bowel preparation for colonoscopy in patients with chronic constipation. BMC Gastroenterol 2021;21(1):387. 9. Parente F, Vailati C, Bargiggia S, et al. 2-Litre polyethylene glycol-citrate-simethicone plus bisacodyl versus 4-litre polyethylene glycol as preparation for colonoscopy in chronic constipation. Dig Liver Dis 2015;47(10):857–63. 10. Sanaka MR, Super DM, Mullen KD, et al. Use of tegaserod along with polyethylene glycol electrolyte solution for colonoscopy bowel preparation: A prospective, randomized, double-blind, placebo-controlled study. Aliment Pharmacol Ther 2006;23(5):669–74. 11. Fukudo S, Miwa H, Nakajima A, et al. High-dose linaclotide is effective and safe in patients with chronic constipation: A phase III randomized, double-blind, placebo-controlled study with a long-term open-label extension study in Japan. Neurogastroenterology Motil 2019;31(1):e13487. 12. Stein DJ, Copland A, McDaniel D, et al. Single-dose linaclotide is equal in efficacy to polyethylene glycol for bowel preparation prior to capsule endoscopy. Dig Dis (Basel, Switzerland) 2019;37(4):297–302. 13. Zhang C, Chen X, Tang B, et al. A novel ultra-low-volume regimen combining 1 L polyethylene glycol and linaclotide versus 2 L polyethylene glycol for colonoscopy cleansing in low-risk individuals: A randomized controlled trial. Gastrointest Endosc 2023;97(5):952–61.e1. 14. Yoshida N, Naito Y, Murakami T, et al. Safety and efficacy of a same-day low-volume 1 L PEG bowel preparation in colonoscopy for the elderly people and people with renal dysfunction. Dig Dis Sci 2016;61(11):3229–35. 15. Lai EJ, Calderwood AH, Doros G, et al. The Boston bowel preparation scale: A valid and reliable instrument for colonoscopy-oriented research. Gastrointest Endosc 2009;69(3 Pt 2):620–5. 16. Calderwood AH, Schroy PC III, Lieberman DA, et al. Boston Bowel Preparation Scale scores provide a standardized definition of adequate for describing bowel cleanliness. Gastrointest Endosc 2014;80(2):269–76. 17. Park JS, Kim MS, Kim H, et al. A randomized controlled trial of an educational video to improve quality of bowel preparation for colonoscopy. BMC Gastroenterol 2016;16(1):64. 18. Liu C, Song X, Hao H. Educational video followed by retelling bowel preparation process to improve colonoscopy bowel preparation quality: A prospective nursing intervention study. Med Sci Monit 2018;24:6029–37. 19. Guo X, Shi X, Kang X, et al. Risk factors associated with inadequate bowel preparation in patients with functional constipation. Dig Dis Sci 2020;65(4):1082–91. 20. Sirinawasatien A, Sakulthongthawin P, Chanpiwat K, et al. Bowel preparation using 2-L split-dose polyethylene glycol regimen plus lubiprostone versus 4-L split-dose polyethylene glycol regimen: A randomized controlled trial. BMC Gastroenterol 2022;22(1):424. 21. Lee J, Jeong SJ, Kim TH, et al. Efficacy of mosapride citrate with a split dose of polyethylene glycol plus ascorbic acid for bowel preparation in elderly patients: A randomized controlled trial. Medicine 2020;99(2):e18702. 22. Guo R, Wang YJ, Liu M, et al. The effect of quality of segmental bowel preparation on adenoma detection rate. BMC Gastroenterol 2019;19(1):119. 23. Choi YI, Lee JJ, Chung JW, et al. Efficacy and patient tolerability profiles of probiotic solution with bisacodyl versus conventional cleansing solution for bowel preparation: A prospective, randomized, controlled trial. J Clin Med 2020;9(10):3286. 24. Hassan C, East J, Radaelli F, et al. Bowel preparation for colonoscopy: European society of gastrointestinal endoscopy (ESGE) guideline–update 2019. Endoscopy 2019;51(8):775–94. 25. Ell C, Fischbach W, Bronisch HJ, et al. Randomized trial of low-volume PEG solution versus standard PEG + electrolytes for bowel cleansing before colonoscopy. Am J Gastroenterol 2008;103(4):883–93. 26. Ponchon T, Boustiere C, Heresbach D, et al. A low-volume polyethylene glycol plus ascorbate solution for bowel cleansing prior to colonoscopy: The NORMO randomised clinical trial. Dig Liver Dis 2013;45(10):820–6. 27. Sey MSL, Von Renteln D, Sultanian R, et al. A multicenter randomized controlled trial comparing two bowel cleansing regimens for colonoscopy after failed bowel preparation. Clin Gastroenterol Hepatol 2022;20(6):e1283–91. 28. Barkun AN, Martel M, Epstein IL, et al. The bowel CLEANsing national initiative: High-volume split-dose vs low-volume split-dose polyethylene glycol preparations: A randomized controlled trial. Clin Gastroenterol Hepatol 2022;20(6):e1469–e1477. 29. Corsetti M, Landes S, Lange R. Bisacodyl: A review of pharmacology and clinical evidence to guide use in clinical practice in patients with constipation. Neurogastroenterology Motil 2021;33(10):e14123. 30. Luthra P, Camilleri M, Burr NE, et al. Efficacy of drugs in chronic idiopathic constipation: A systematic review and network meta-analysis. Lancet Gastroenterol Hepatol 2019;4(11):831–44. 31. Ahsan MK, Tchernychev B, Kessler MM, et al. Linaclotide activates guanylate cyclase-C/cGMP/protein kinase-II-dependent trafficking of CFTR in the intestine. Physiol Rep 2017;5(11):e13299. 32. Jung YS, Lee CK, Eun CS, et al. Low-volume polyethylene glycol with ascorbic acid for colonoscopy preparation in elderly patients: A randomized multicenter study. Digestion 2016;94(2):82–91. 33. Zhang M, Zou W, Xu C, et al. Polyethylene glycol combined with linaclotide is an effective and well-tolerated bowel preparation regimen for colonoscopy: An endoscopist-blinded, randomized, controlled trial. Eur J Gastroenterol Hepatol 2021;33(1S Suppl 1):e625–e633. 34. Li Y, Jia X, Liu B,
Comments (0)