
Remember me









The global incidence of gastric cancer has been declining steadily over the past few decades, which is attributed to improvement in socioeconomic conditions, identification and eradication of Helicobacter pylori infection, and utilization of screening in some high-risk countries (1–3). Nevertheless, according to the Global Cancer Statistics 2020 report by the International Agency for Research on Cancer, gastric cancer continues to account for 5.6% of all new cancer cases (ranking fifth in incidence) and 7.7% of all cancer deaths (ranking fourth in mortality), highlighting its impact on cancer burden (4). In recent years, several studies have demonstrated a rise in gastric cancer among young adults, which raises interest in improving early detection among this group of younger individuals (5,6). However, a recent study showed that despite the increase in the total number of new cases of young gastric cancer, the age-standardized incidence has been decreasing (7).
Unlike colorectal cancer, there is no universally accepted definition for young-onset gastric cancer, as cutoff age ranges from 30 to 50 years have been used, varying across different studies (8–10). In certain studies, young-onset gastric cancer is defined as occurring before the age of 40, while in others, the definition generally encompasses all patients diagnosed before the age of 45 or 50 years (6,11–13).
Given various limitations including the appropriate cutoff age for young-onset gastric cancer, the prognosis for these patients remains controversial. As the most prevalent histological type of gastric cancer, the clinicopathological characteristics of gastric carcinoma have been observed to differ between younger and older patients, leading to the general belief that younger patients may experience a worse prognosis due to delayed diagnosis or more aggressive tumor behavior (14–16). The majority of current research on the clinicopathological characteristics of young-onset gastric carcinoma has been conducted in single-center studies. These studies are primarily in East Asian countries, such as Japan, South Korea, and China, with limited sample sizes (8,17,18). However, a comprehensive systematic summary of the clinicopathological features specific to patients with young gastric carcinoma at the global level is lacking.
Generally, the progression of gastric carcinoma, particularly intestinal-type adenocarcinoma, follows a well-defined and identifiable cascade of events that includes progression from inflammation to atrophy, intestinal metaplasia, dysplasia, and eventually carcinoma (3,19,20). This disease is closely associated with environmental factors, dietary habits, genetic mutations, and epigenetic changes. Efforts to enhance screening programs and facilitate early detection and treatment of gastric carcinoma are crucial, and prioritizing proactive measures to address preventable factors contributing to the development of this disease is imperative. Thus far, research on risk factors of young-onset gastric carcinoma remains limited, other than the World Health Organization's (WHO) comprehensive listing of factors such as H. pylori infection, salty fish, and alcohol use (21–23).
This is a comprehensive systematic review and meta-analysis of global studies pertaining to young-onset gastric carcinoma spanning from 1990 to 2023. We aimed to provide a comprehensive summary of the clinicopathological characteristics specific to this population and to identify risk factors associated with young-onset gastric carcinoma.
METHODS Search strategyThis systematic review and meta-analysis followed the Meta-analyses Of Observational Studies in Epidemiology guidelines (24). We searched PubMed, EMBASE, Web of Science, and MEDLINE for all observational studies, including cohort studies or cross-sectional studies, published between January 1, 1990, and September 1, 2023, without language restriction. To obtain a more comprehensive outcome and minimize the impact resulting from the selected age threshold, we have chosen 50 years as the cutoff age for young-onset gastric carcinoma in this study to encompass a broader study population. The primary search terms included the following related to gastric carcinoma (e.g., “Gastric Neoplasm,” “Gastric Carcinoma,” “Stomach Carcinoma,” “Stomach Neoplasm”) and our targeted population (e.g., “young,” “young onset,” “early onset”). Detailed search strategies for each database are shown in Supplementary Digital Content (see Supplementary Table 1, https://links.lww.com/CTG/B123). Study types that were excluded from this review were meta-analyses, systematic reviews, conference papers, editorials, case reports, and animal experimental studies. The search was not restricted by language or region. This systematic review and meta-analysis were registered with PROSPERO (CRD42023466131). We used the EndNote X9 (Clarivate, Philadelphia, PA) for literature management.
The clinical characteristics investigated in this study included the following: patient's sex, symptoms at presentation (substratified into abdominal pain, anorexia/weight loss, dyspepsia/vomiting/nausea/early satiety, dysphagia, and gastrointestinal bleeding), tumor location (cardia vs non-cardia), functional regions (body, fundus, antrum, angular incisure, and multifocal (whole gastric)), and anatomical regions (proximal, middle, distal, or overlapping) (25). The pathological features included the Lauren histological classification, WHO histological classification, and degree of differentiation (26,27). The risk factors considered included positive family history of gastric cancer, H. pylori infection, high consumption of sodium-rich or other detrimental foods (refers to more frequent intake of beef and canned, smoked, and salted food and less frequent intakes of fresh fruit/vegetables as suggested by Chung et al (28)), alcohol intake, obesity, and smoking. Stratified analyses were conducted based on age (≤30 years vs 31–50 years), sex groups, Asian or non-Asian countries, and countries with national gastric cancer screening programs (Japan and South Korea) vs those without. Studies that reported survival outcomes (including 1-, 3-, and 5-year overall survival rates) for young-onset gastric carcinoma were also documented.
Exclusion criteria were set as (i) studies that set the cutoff age of young-onset gastric carcinoma over 50 years, (ii) included data from specific study populations (e.g., pregnant, hereditary carcinoma, or patients with other specific chronic diseases [such as comorbidity with inflammatory bowel diseases]), (iii) studies solely conducted in a single pathological type (e.g., exclusively focusing on signet ring cell carcinoma), and (iv) studies investigated among pathological types other than carcinoma (e.g., neuroendocrine tumor, lymphoma, sarcoma). Eligible studies presented the raw data as either a proportion (or odds ratio [OR] for risk factors) with confidence interval (CI) or SE or provided sufficient information to calculate the CI, such as total sample size. The Wilson score interval method, an extension of the normal approximation to account for the loss of coverage typical in Wald intervals, was used to calculate all CIs not described in the original articles (29).
Data extraction and quality assessmentThe studies obtained from the databases were stored in the reference management software EndNote. The EndNote search function was used for extracting relevant studies before screening the citations against the inclusion and exclusion criteria by 2 independent authors (Y.H.L. and J.F.). In cases where duplicates or publications from the same study were identified, preference was given to selecting the more recent publication or the one with greater detail for inclusion in the review. A third investigator (W.K.L.) mediated any discrepancies in article inclusion or data extraction. Data extracted included the authors' names, publication year, sample collection period (year), lesion location, number of participants, average age (or age scale), study settings (hospital, regional/community, or national registry-based), clinicopathological information, and risk factors and their related ORs (with 95% CIs) (see Supplementary Tables 2 and 3, https://links.lww.com/CTG/B123). Studies were not included if full-text articles were unable to be obtained from all sources including direct contact with the authors. Studies published in languages other than English were translated with Google Translate. To verify the accuracy of the critical data for statistical analysis, we have listed the assistance of proficient users of these languages. Funnel plot and Egger's test were used to assess the presence of publication bias for the H. pylori infection rate and proportion of positive gastric cancer family history.
Two independent authors (Y.H.L. and J.F.) performed quality assessments as recommended by Loney et al (30). The intact quality assessment procedure has a maximum score of 8 points, encompassing 3 key aspects: valid study methods, result interpretation, and result applicability. Disagreement on quality assessment score was settled with discussion. Studies with a quality assessment score of 50% or above were included in the final meta-analysis. Detailed information about the quality assessment and study settings of the included research are presented in Supplementary Table 4, https://links.lww.com/CTG/B123.
Statistical analysisThe pooled proportions or the OR and corresponding 95% CI were calculated using either the inverse-variance fixed-effects model or the DerSimonian and Laird random-effects model, based on the estimation of heterogeneity variance (31,32). The selection of the random-effects model and fixed-effects model was determined by I2 values, with a threshold of ≥50% for the random-effects model and fixed-effects model. The pooled OR was excluded if it was calculated based on fewer than 3 studies. Heterogeneity was assessed by using the I2 index and Cochran Q test. A P value of less than 0.05 between subgroups implied that the element is a source of heterogeneity. High between-study heterogeneity (I2 > 75%) was investigated using a leave-one-out method for sensitivity analysis and subgroup analysis (33,34). To evaluate the significance between the 2 groups, we assessed the coverage of pooled 95% CI (35). The temporal trend of the H. pylori infection rate was evaluated by the midpoint of the sample collection time and the infection rate of individual studies, using a generalized linear model. Statistical analyses were performed by using Stata (version 17.0; Stata Corp, College Station, TX) and R software (version 4.2.1, package: binom, ggplot2).
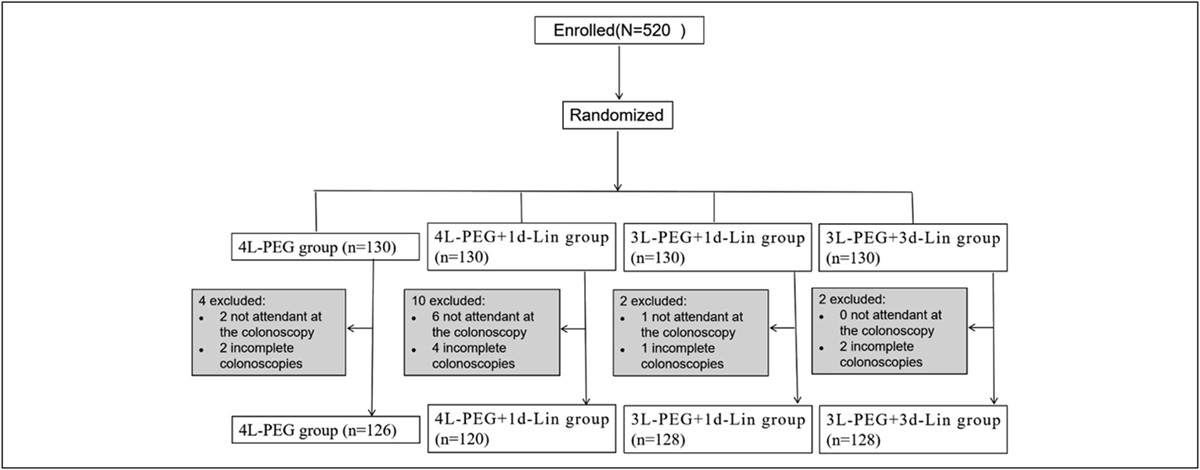
RESULTSA total of 5,696 articles published between January 1, 1990, and September 1, 2023, were identified after the initial search. The first stage excluded 2,369 duplicate records by the literature manager; 2,035 duplicate records, unrelated articles, or animal experiments were further removed manually. A total of 1,292 full texts were reviewed for quality assessment, with 1,208 articles further excluded as per exclusion criteria defined above. Ultimately, 84 studies (with publication years ranging from 1992 to 2023) from 18 countries or regions were included for analysis, including 9 studies that reported risk factors of young-onset gastric carcinoma (Figure 1). Most of the included studies (54 studies, 64.3%) were conducted in Asia, particularly China (24 studies, 28.6%), South Korea (15 studies, 17.9%), and Japan (15 studies, 17.9%). The majority (60 studies, 71.4%) were hospital-based studies, followed by 15 (17.9%) national registry-based studies and 9 (10.7%) regional/community registry-based studies. The quality of the included studies was relatively high according to the quality assessment results (points scale: 4–7, average points: 6.6) (see Supplementary Table 4, https://links.lww.com/CTG/B123).
 Figure 1.:
Figure 1.: Flowchart for study selection following the Meta-analyses Of Observational Studies in Epidemiology (MOOSE) guidelines.
Clinicopathological characteristicsYoung-onset gastric carcinoma cases have a slight female predominance (53.7%, 95% CI: 51.6%–55.7%) than male (46.4%, 95% CI: 44.3%–48.4%). Most of the patients in the included studies were symptomatic (87.0%, 95% CI: 82.4%–91.7%), with symptoms including abdominal pain (61.9%, 95% CI: 54.2–69.7), anorexia/weight loss (29.9%, 95% CI: 17.5%–42.2%), dyspepsia-associated symptoms (vomiting, nausea, or early satiety) (24.6%, 95% CI: 16.7–32.5), dysphagia (18.5%, 95% CI: 10.4%–26.6%), and gastrointestinal bleeding (or with anemia) (14.1%, 95% CI: 8.9%–19.3%) (Table 1 and see Supplementary Figures 1–2, https://links.lww.com/CTG/B123).
Table 1. - Clinicopathological characteristics of young-onset gastric carcinoma ( Clinicopathological characteristics No. of studies No. of patients Estimated proportion (95% CI)b P heterogeneity/I 2 P between groups Positive family history of gastric cancer 27 3,562 12.1% (9.5–14.7) <0.001/86.1% At least in 1 first-degree relative 5 516 8.3% (5.0–11.6) 0.031/62.5% Symptomatic 13 1,906 87.0% (82.4–91.7) <0.001/94.8% Sex ratio <0.001 Male 62 7,499 46.4% (44.3–48.4) <0.001/80.1% Female 62 7,967 53.7% (51.6–55.7) <0.001/80.2% Symptoms <0.001/98.1% <0.001 Abdominal pain 20 1885 61.9% (54.2–69.7) <0.001/92.9% Anorexia/weight loss 12 1,176 29.9% (17.5–42.2) <0.001/97.6% Dyspepsia/vomiting/nausea/early satiety 16 1,517 24.6% (16.7–32.5) <0.001/97.4 Dysphagia 9 897 18.5% (10.4–26.6) <0.001/94.4% GIB (melena/hematemesis/anemia) 11 1,105 14.1% (8.9–19.3) <0.001/89.6% Topography <0.001 Cardia carcinoma 12 541 10.7% (4.6–16.9) <0.001/97.6% Non-cardia carcinoma 12 4,520 89.3% (83.2–95.5) <0.001/97.6% Anatomical location <0.001 Proximal 33 5,174 17.2% (14.4–20.0) <0.001/87.6% Middle 33 5,056 30.3% (25.7–35.0) <0.001/93.2% Distal 33 5,014 46.0% (41.2–50.7) <0.001/91.7% Multifocal (whole gastric) 19 3,222 6.1% (4.4–7.8) <0.001/75.7% Overlapping/NOS 1 760 17.9% (19.3–20.8) — Functional region <0.001 Fundus 6 510 6.8% (2.3–11.4) 0.004/71.3% Body 14 5,296 40.6% (30.1–51.1) <0.001/97.6% Angular incisure 3 398 7.6% (4.5–10.6) 0.286/20.1% Antrum 14 5,205 41.3% (33.5–49.2) <0.001/95.7% Multifocal 16 5,554 11.9% (7.6–16.3) <0.001/96.3% Lauren classification <0.001 Diffuse type 38 4,564 71.1% (66.8–75.3) <0.001/90.9% Intestinal type 38 1,522 21.4% (17.3–25.5) <0.001/93.0% Mixed type 24 725 10.9% (8.1–13.7) <0.001/89.5% WHO classification <0.001 Tubular/papillary adenocarcinoma 12 5,340 65.1% (57.0–73.3) <0.001/96.5% Signet-ring cell carcinoma 18 2,973 31.3% (23.7–38.9) <0.001/97.6% Mucinous cell carcinoma/others 13 6,721 3.9% (2.6–5.3) <0.001/69.8% Differentiation <0.001 Poorly/undifferentiated 46 7,963 81.9% (79.7–84.2) <0.001/87.9% Well/moderately differentiated 46 1,516 15.6% (13.7–17.5) <0.001/83.7% Helicobacter pylori infection rate (%) 5,213 60.0% (47.1–72.8) 0.836/98.7% <0.001 Histology 4 273 61.5% (27.5–95.4) <0.001/98.1% Mixed methodsa 5 376 63.2% (37.2–89.2) <0.001/97.5% RUT 3 263 69.3% (45.9–92.7) <0.001/93.7% Serology 3 3,404 60.7% (14.3–97.2) <0.001/99.5% Not mentioned 5 897 49.6% (26.5–72.7) <0.001/98.4%CI, confidence interval; GIB, gastrointestinal bleeding; NOS, not otherwise specified; RUT, rapid urease test; WHO, World Health Organization.
aMixed methods represented more than 2 methods mentioned in the original studies.
bThe random or fixed-effects model calculated pooled proportion (and 95% CI).
Non-cardia carcinoma (89.3%, 95% CI: 83.2%–95.5%) was significantly more common than cardia carcinoma (10.7%, 95% CI: 4.6%–16.9%; Table 1). Based on anatomical categorization, the proportion of gastric carcinoma in the distal region (41.4%, 95% CI: 33.3%–49.6%) and middle region (30.3%, 95% CI: 25.7%–35.0%) was higher than in proximal or multifocal lesions. In terms of functional categorization, tumors were more commonly located in the antrum (41.3%, 95% CI: 33.5%–49.2%) and corpus (40.6%, 95% CI: 30.1%–51.1%; Table 1 and see Supplementary Figure 3, https://links.lww.com/CTG/B123).
Most of the cases of young-onset gastric carcinoma were characterized as poorly differentiated or undifferentiated (81.9%, 95% CI: 79.7%–84.2%), with a small proportion of well or moderately differentiated lesions (15.6%, 95% CI: 13.7%–17.5%; Table 1 and see Supplementary Figure 4, https://links.lww.com/CTG/B123). For Lauren histological classification, diffuse-type carcinoma (71.1%, 95% CI: 66.8%–75.3%) was significantly more prevalent than intestinal type (21.4%, 95% CI: 17.3%–25.5%) and mixed type (10.9%, 95% CI: 8.1%–13.7%; see Supplementary Figures 4–2). Regarding the WHO classification, tubular or papillary adenocarcinoma accounted for the highest proportion of carcinomas (65.1%, 95% CI: 57.0%–73.3%), followed by signet-ring cell carcinoma (31.3%, 95% CI: 23.7%–38.9%) and mucinous cell adenocarcinoma (3.9%, 95% CI: 2.6%–5.3%, see Supplementary Figures 4–3, https://links.lww.com/CTG/B123).
Risk factors of young-onset gastric carcinomaThe pooled proportion of patients with a positive family history of gastric cancer was 12.1% (95% CI: 9.5%–14.7%) while the pooled rate of H. pylori infection was 60.0% (95% CI: 47.1%–72.8%; Table 2 and Figure 2a). The pooled H. pylori infection rate showed a decline over the past 3 decades (Figure 2b). The current H. pylori infection rate (66.3%, 95% CI: 48.9%–83.6%; tested by histology or rapid urease test) was higher compared with the infection rates obtained through other diagnostic methods (55.8%, 39.6%–72.0%). Further stratified analysis based on different diagnostic methods revealed that studies based on the rapid urease test reported the highest rate of H. pylori infection of 69.3% (95% CI: 45.9%–92.7%). The reported proportion of positive family history of gastric cancer (PEgger's test <0.001) and H. pylori infection rate (PEgger's test = 0.017) showed significant publication bias but remained stable after sensitivity analysis (see Supplementary Figure 7, https://links.lww.com/CTG/B123).
Table 2. - Estimated pooled odds ratio of risk factors of young-onset gastric carcinoma Risk factors No. of studies Study population Estimated odds ratio (95% CI) P heterogeneity I 2 Positive family history of gastric cancer 3 6,534 4.0 (2.8–5.2) 0.760 0% H elicobacter pylori infection 7 6,718 2.3 (1.4–3.2) 0.001 72.8% Salty food or other high-risk dieta 3 6,563 2.1 (1.3–2.8) 0.008 59.3% Alcohol intake 4 6,559 2.0 (1.3–2.6) 0.047 62.2% Smoking 5 7,295 1.5 (0.6–2.3) <0.001 64.9% Obesityb 4 1,309 1.7 (1.5–2.0) 0.322 14.0%CI, confidence interval.
aRefers to more frequent intake of beef and canned, smoked, and salted food and less frequent intake of fresh fruit/vegetables.
bCutoff value: body mass index ≥35 kg/m2 (2 studies); body mass index ≥30 kg/m2 (2 studies).
 Figure 2.:
Figure 2.: Pooled Helicobacter pylori infection rate of young-onset gastric carcinoma (a); temporal trend of H. pylori infection rate (b). The bubble area represents the number of subjects included in an individual report. The bubble's position was determined by the study year of the report (midpoint year of the study period) and the infection rate. The bubble's color was determined by the diagnostic methods. The fitted curve was drafted to show the time trend of infection rate (default method: generalized linear model [glm]). RUT, rapid urease test.
Nine studies reported on risk factors of young-onset gastric carcinoma. Among the 6 risk factors, positive family history of gastric cancer was found to have the highest OR associated with the development of gastric carcinoma in young individuals (pooled OR: 4.0; 95% CI: 2.8–5.2), followed by H. pylori infection (pooled OR: 2.3; 95% CI: 1.4–3.2; see Supplementary Figure 8, https://links.lww.com/CTG/B123). As for dietary or behavioral risk factors, intake of salty food or other high-risk diets was found to have a pooled OR of 2.1 (95% CI: 1.3–2.8), followed by alcohol consumption (pooled OR: 1.9, 95% CI: 1.3–2.6), smoking (pooled OR: 1.5, 95% CI: 0.6–2.3), and obesity (pooled OR: 1.7, 95% CI: 1.5–2.0). The pooled OR of positive H. pylori infection remained stable after sensitivity analysis, despite the presence of high heterogeneity (I2 = 72.8%). Other risk factors demonstrated relatively low to middle-level heterogeneity (I2 < 70%).
Age, sex, and regional-stratified analysisVery early-onset carcinoma (age ≤30 years) constitutes 20.5% (95% CI: 17.6%–23.4%) of all young-onset carcinoma cases (see Supplementary Table 5 and Supplementary Figure 9, https://links.lww.com/CTG/B123). In this subgroup of very early-onset carcinoma, the proportion of undifferentiated tumors was higher (94.5%, 95% CI: 84.9–99.0%) than in the 31–50 years age group (83.7%, 95% CI: 74.2%–94.5%), based on 2 studies with relevant data. The Lauren type classification in different age groups was only reported in one study by Li et al (36), which revealed a significantly higher proportion of diffuse histological type and a lower proportion of mixed type among individuals aged 30 years and older (see Supplementary Figure 10, https://links.lww.com/CTG/B123).
When considering the patient's sex, both sexes exhibited similar functional and anatomical tumor distribution. Female patients were, however, found to have a higher proportion of poor/undifferentiated tumor histology compared with male patients (91.2%, 95% CI: 87.1%–95.3% vs 72.8%, 95% CI: 63.8%–81.8%). Although both sexes shared a comparable distribution of WHO histological classification subtypes, female patients demonstrated a higher proportion of diffuse-type tumors than male patients (82.2%, 95% CI: 74.7%–89.6% vs 72.2%, 95% CI: 61.9%–82.0%, respectively; Table 3 and see Supplementary Figures 11–12, https://links.lww.com/CTG/B123). Female patients also had a higher prevalence of positive family history of gastric cancer compared with male patients (15.6%, 95% CI: 1.8%–29.4% vs 12.6%, 95% CI: 2.7%–22.5%). The infection rate of H. pylori was also higher in female patients compared with male patients (85.7%, 95% CI: 73.8%–97.6% vs 73.3%, 95% CI: 56.3%–90.4%), although this was only reported in a single study by Ławniczak et al (37). Limited studies investigated the sex-stratified OR of various risk factors, and male patients had higher exposure to risk factors including alcohol, smoking, and H. pylori infection than female patients (see Supplementary Figure 13, https://links.lww.com/CTG/B123).
Table 3. - Sex-stratified analysis on clinicopathological characteristic of young-onset gastric carcinoma Clinicopathological characteristics Sex No. of studies Study population Estimated pooled proportion (95% CI) P heterogeneity I 2 Anatomical regions Antrum Male 2 437 62.3% (57.8–66.8) 0.728 0.00% Female 2 391 57.3% (52.5–62.2) 0.553 0.00% Corpus Male 2 437 21.7% (8.2–35.2) 0.002 89.30% Female 2 391 20.7% (0.8–42.1) <0.001 96.00% Multifocal Male 2 437 8.1% (0.8–16.9) 0.019 81.90% Female 2 391 17.0% (0.3–39.0) <0.001 94.30% Functional regions Proximal Male 4 205 8.8% (4.8–12.8) 0.712 0.00% Female 4 170 7.6% (3.5–11.8) 0.392 0.00% Middle Male 4 205 38.6% (27.7–49.5) 0.052 61.20% Female 4 198 37.8% (22.0–53.5) <0.001 83.60% Distal Male 4 205 47.2% (32.0–62.4) 0.002 79.90% Female 4 198 48.1% (29.6–66.7) <0.001 87.90% Multifocal Male 4 205 3.0% (0.4–5.7) 0.636 0.00% Female 4 198 6.2% (2.6–9.8) 0.923 0.00% Differentiation Well/moderate differentiated Male 6 639 27.2% (18.2–36.2) <0.001 81.10% Female 6 626 8.8%
Comments (0)