
Remember me









Irritable bowel syndrome (IBS) is a chronic functional gastrointestinal (GI) disorder that affects approximately 10%–20% of the population (1). Approximately 40% of patients with IBS are diarrhea predominant (IBS-D) characterized by abdominal pain associated with diarrhea (2). IBS-D seriously impairs patients' quality of life, work activities, and social function (3). However, the pathogenesis of IBS-D is not fully understood, and current treatment options are limited, leading to poor patients' satisfaction. The pathophysiology of IBS-D is complex and involves multiple factors, such as dysfunction of gut-brain interaction, altered GI sensory and motor functions, mucosal low-grade inflammation, impaired intestinal barrier function, and gut microbiota dysbiosis (4,5).
Current evidence has confirmed that the human gut microbiota plays a key role in the pathogenesis of IBS-D (6). It can modulate many important physiological processes, including metabolism of bile acids (BAs), short-chain fatty acid, amino acids, etc (7). Moreover, the gut microbiota can affect GI motility and secretion, mucosal inflammation, intestinal permeability, and even the interaction between the gut and the brain (8,9). A number of studies have reported that patients with IBS-D have different microbial community composition in the fecal samples with healthy individuals (10). For example, the Firmicutes:Bacteroidetes ratio at the phylum level is increased and the relative abundance of Bifidobacterium and Lactobacillus genera is decreased in the feces of patients with IBS-D (11–13). However, most studies have focused on the fecal microbiota; the mucosa-associated microbiota (MAM) is not as frequently studied in IBS-D. This might be partly due to the lower microbial density in the mucosa than in the feces, which makes it difficult to get enough bacterial DNA to analyze (14). MAM is closer to the host cells and more stable than fecal microbiota (15,16). A few studies have attempted to evaluate MAM and found that patients with IBS-D had a lower microbial evenness (not richness) in the sigmoid colon compared with HCs, and the abundance of Streptococcus, Acidaminococcus, Butyricicoccus, and Parvimonas at the genus level was higher in patients with IBS-D (15). Another research reported that the defecation frequency was negatively correlated with the number of Bifidobacteria and Lactobacilli in the rectal MAM, suggesting that host-microbiome interactions were related to the symptom generation in IBS (17). Therefore, it might be more valuable to explore the MAM to better understand the pathophysiology of IBS-D.
Notably, we found in the clinical practice that some patients with IBS-D had multiple small nodules on the mucosal surface of the terminal ileum, where existed abundant lymphoid follicles. According to some previous studies, this phenomenon with multiple benign nodules (2–10 mm in diameter) is defined as nodular lymphoid hyperplasia (NLH), indicating a mucosal low-grade inflammation (18,19). Moreover, evidence has shown that there was a dysbiosis in the mucosa of the terminal ileum in patients with NLH, and the relative abundance of Bacteroides was decreased while that of some opportunistic pathogens was increased (20). All these results suggest that patients with IBS-D may display a mucosal dysbiosis in the terminal ileum. To examine this hypothesis, we explored the terminal ileal MAM in patients with IBS-D and HCs and its correlation with abdominal and psychological symptoms.
MATERIALS AND METHODS ParticipantsA total of 60 participants were recruited in Renji Hospital from January 2022 to January 2023, including 32 patients with IBS-D and 28 healthy controls (HCs). All subjects had voluntarily signed an informed consent form before entry. The inclusion and exclusion criteria were as follows:
Inclusion criteria of patients with IBS-D were as follows: (i) aged 18–55 years; (ii) patients with IBS-D diagnosed by the ROME-IV criteria: recurrent abdominal pain associated with diarrhea, occurring at least 1 day a week for the last 3 months and lasting more than 6 months; and (iii) having no organic lesions in the colonoscopy examination, B-scan ultrasound, electrocardiography, chest radiography, blood cell counts, and coagulation tests. Inclusion criteria of HCs were as follows: (i) aged 18–55 years; (ii) having no history of organic diseases; and (iii) having no organic lesions in the colonoscopy examination, B-scan ultrasound, electrocardiography, chest radiography, blood cell counts, and coagulation tests.
Exclusion criteria: (i) colonoscopy examination showed intestinal ulcer, erosion, bleeding, active inflammation, colonic polyps, dysplasia, or suspicious malignant lesions; (ii) having a history of other overlapping digestive diseases (GI infection, inflammatory bowel disease, celiac diseases, or tumors); (iii) having organic diseases of circulatory, respiratory, hepatic, or renal systems; (iv) having a history of gallstones or cholecystectomy; (v) taking antibiotics, probiotics, prokinetics, proton pump inhibitors, or any other drugs that affect the gut microbiota within 6 months; and (vi) planned pregnancy, pregnant, or breastfeeding.
Interventions and blindnessDedicated gastroenterologists enrolled participants, obtained informed consent, and collected clinical data, including demographic data, defecation frequency (DF), the degree of abdominal pain, the severity of IBS-D, and the degree of anxiety and depression. DF meant the frequency of stools per day during recruitment. The degree of abdominal pain was evaluated by a visual analog scale (VAS, 10 cm) score (21). And the severity of IBS-D was assessed by IBS Severity Scoring System (IBS-SSS) (22), including pain severity, pain frequency, severity of abdominal distension, bowel habit dissatisfaction, and daily life interference, ranging from 0 to 100 points for each item. The degree of anxiety and depression were evaluated by the Generalized Anxiety Disorder Questionnaire (GAD-7) and Patient Health Questionnaire (PHQ-9) scores (23,24), containing 7 items and 9 items on a 4-point (0–3) scale, respectively.
During recruitment, our gastroenterologists had provided dietary instructions to all participants, including the following:
To have regular meals and not to skip meals (3 meals per day); To have moderate portion of meals, including proper intake of carbohydrates, fats, and fiber; To have moderate intake of fresh fruit; To reduce the consumption of spicy foods; To drink almost 2 L of water per day; and To reduce coffee, tea, fizzy, or alcohol drinks.Participants followed these dietary instructions and underwent colonoscopy 2 weeks later in Renji Hospital. All participants received 4 L of polyethylene glycol electrolyte lavage solution as bowel preparation 1 day before colonoscopy.
Our endoscopists were blinded to the clinical status during colonoscopy. Two mucosal biopsy samples of the terminal ileum were obtained for further mucosal microbial profiling. In addition, 1 mucosal biopsy sample was fixed in formalin for histological analysis. Dedicated histopathologists, also blinded to the clinical status, assessed the histological features.
Moreover, IBS-D subgroups were identified by both endoscopic and histological features, including the IBS-D with NLH subgroup (existence of multiple small nodules on the mucosal surface of the terminal ileum with a histological feature of lymphoid follicular hyperplasia) and the IBS-D without NLH subgroup.
16S rRNA gene sequencingMicrobial DNA was extracted from the mucosal biopsy samples using the OMEGA Soil DNA Kit (M5635-02) (Omega Bio-Tek, Norcross) following the manufacturer's instructions. Extracted DNA quantity was measured using a NanoDrop NC2000 spectrophotometer (Thermo Fisher Scientific, Waltham, MA), and DNA quality was determined by 1% agarose gel electrophoresis. Then the hypervariable V3-V4 region of the bacterial 16S ribosomal RNA (rRNA) gene was amplified using primers 338F (5'-ACTCCTACGGGAGGCAGCA-3') and 806R (5'-GGACTACHVGGGTWTCTAAT-3'). Then amplicons were further purified using Vazyme VAHTSTM DNA Clean Beads (Vazyme, Nanjing, China) and quantified using the Quant-iT PicoGreen and dsDNA Assay Kit (Invitrogen, Carlsbad, CA). After the library was constructed, sequencing was performed using the Illumina NovaSeq platform with NovaSeq 6000 SP Reagent Kit (500 cycles) by Shanghai Metabo-Profile Biotechnology (Shanghai, China).
Bioinformatics analysisRaw sequence data were demultiplexed using the demux plugin, followed by primer cutting with cutadapt plugin. Then sequences were quality filtered, denoised, merged, and chimera removed using the DADA2 plugin. Sequences with dereplication were defined as amplicon sequence variants. Taxonomy was assigned to amplicon sequence variants using the classify-sklearn naive Bayes taxonomy classifier in feature-classifier plugin against the Greengenes 13_8 99% Operational Taxonomic Units reference sequences. Sequence data analysis was mainly performed using QIIME2 and R packages (V3.2.0). Alpha diversity was analyzed, including Chao1, Observed species, and Shannon indexes. Beta diversity analysis was performed using Bray-Curtis metrics and Jaccard metrics and visualized through principal coordinate analysis (PCoA). The significance of differentiation of microbial composition between the 2 groups was assessed by ADONIS (PERMANOVA, permutational multivariate analysis of variance) using QIIME2. The linear discriminant analysis (LDA) effect size (LEfSe) was used to identify significantly different bacterial taxa between patients with IBS-D and HCs (The LEfSe P value < 0.05 and the LDA score threshold > 2.0).
The primary microbiome end point was to compare microbial composition between the IBS-D group and the HC group, including alpha and beta diversity analyses and LEfSe analysis. The secondary microbiome end point was to compare microbial composition among the IBS-D with NLH subgroup, IBS-D without NLH subgroup, and the HC group.
Statistical analysisData were presented as the mean ± standard error of measurement. The independent sample t test and the nonparametric Mann-Whitney U test were used to compare measurement data in the 2 groups, and the χ2 test was used to analyze qualitative data. Statistical analysis was performed using SPSS version 26.0 (SPSS). Values of P < 0.05 were considered statistically significant. Moreover, the Spearman correlation analysis was performed to examine the associations between the relative abundance of mucosal microbiota and clinical parameters in the IBS-D group.
This study has been approved by the ethics committee of Renji Hospital, Shanghai Jiaotong University School of Medicine (Approval No. KY-2019072).
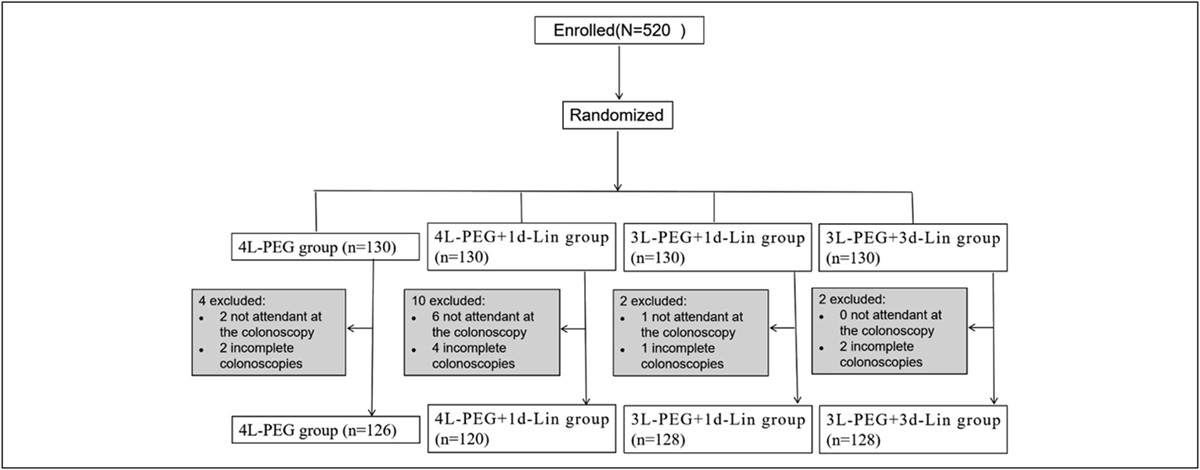
RESULTS Participants’ characteristicsA total of 32 patients with IBS-D and 28 HCs were recruited. In the IBS-D group, 2 cases were excluded because of the lack of laboratory examinations, 2 cases failed to enter the lumen of the terminal ileum during colonoscopy, and 3 cases had colonic polyps observed during colonoscopy. And in the HC group, 1 case was excluded because of the lack of laboratory examinations, 1 case failed to enter the lumen of the terminal ileum during colonoscopy, and 1 case had colonic polyps observed during colonoscopy. Finally, mucosal biopsies from 25 patients with IBS-D and 25 HCs were collected for subsequent 16S rRNA sequencing and statistical analysis. The flow diagram is shown in Figure 1, and participants' characteristics are summarized in Table 1. There were no significant differences in demographic parameters (age, gender, and body mass index) between the 2 groups (P > 0.05). The mean duration of disease in patients with IBS-D was 23.84 ± 3.87 months. The mean VAS score was 4.20 ± 0.33, and the mean IBS-SSS score was 219.00 ± 21.28 in the IBS-D group. Patients with IBS-D had significantly higher DF (1.12 ± 0.07 vs 5.20 ± 0.38), GAD-7 (1.96 ± 0.20 vs 7.72 ± 0.61), and PHQ-9 (1.04 ± 0.15 vs 4.04 ± 0.27) scores compared with HCs (P < 0.01).
 Figure 1.:
Figure 1.: Flow diagram of participants' recruitment. HC, healthy control; IBS-D, diarrhea-predominant irritable bowel syndrome.
Table 1. - Participants' characteristics Characteristics HC IBS-D P N 25 25 — Gender (male/female) 13/12 15/10 0.776 Age (y) 35.84 ± 1.01 33.44 ± 1.29 0.149 BMI (kg/m2) 23.03 ± 0.53 22.52 ± 0.55 0.508 Defecation frequency (d) 1.12 ± 0.07 5.20 ± 0.38a 0.000 Duration of disease (m) — 23.84 ± 3.87 — VAS — 4.20 ± 0.33 — IBS-SSS — 219.00 ± 21.28 — GAD-7 1.96 ± 0.20 7.72 ± 0.61a 0.000 PHQ-9 1.04 ± 0.15 4.04 ± 0.27a 0.000BMI, body mass index; GAD-7, Generalized Anxiety Disorder Questionnaire; HC, healthy control; IBS-D, diarrhea-predominant irritable bowel syndrome; IBS-SSS, IBS, Severity Scoring System; PHQ-9, patient health questionnaire; VAS, visual analog scale.
Data are expressed as mean ± standard error of measurement. Differences between 2 groups were evaluated by independent sample t test or Mann-Whitney U test for measurement data and the χ2 test for qualitative data.
aP < 0.01 compared with the HC group.
Moreover, according to the endoscopic and histological features, patients with IBS-D were divided into IBS-D with NLH (n = 10, 40.0%) and IBS-D without NLH (n = 15, 60.0%) subgroups. All patients with IBS-D with NLH (n = 10) displayed multiple small nodules on the mucosal surface of the terminal ileum on colonoscopy, with the lymphoid follicular hyperplasia on histology, indicating a mucosal low-grade inflammation. The HCs did not have evidence of NLH. The endoscopic images and histological characteristics in patients with IBS-D with or without NLH and in HCs are shown in Figure 2.
 Figure 2.:
Figure 2.: Endoscopic images and pathological characteristics of the terminal ileum in patients with IBS-D with or without NLH and in HCs. Endoscopic images of the terminal ileum from a healthy control (a), a patient with IBS-D without NLH (b), and a patient with IBS-D with NLH (c). Histological characteristics of the terminal ileum from a healthy control (d), a patient with IBS-D without NLH (e), and a patient with IBS-D with NLH (f). HC, healthy control; IBS-D, diarrhea-predominant irritable bowel syndrome; NLH, nodular lymphoid hyperplasia.
Alpha diversity and beta diversity analysesWe performed 16S rRNA gene sequencing of the mucosal biopsy samples from 25 patients with IBS-D and 25 HCs. An average of 83,783 high-quality sequences per sample were obtained, and an average of 91 taxonomic units per sample were generated. The alpha diversity of the MAM in the terminal ileum was lower in the IBS-D cohort than in HCs. Specifically, the Chao1 and Observed species analyses showed a decreased mucosal microbiota richness in patients with IBS-D compared with HCs (P < 0.05). And the Shannon analysis showed significant lower microbial diversity and evenness in the IBS-D group (P < 0.05). The results of the alpha diversity analysis are shown in Figure 3a–c. As to the beta diversity, visualized PCoA based on Bray-Curtis metrics and Jaccard metrics revealed that the overall mucosal microbial profile clustered separately in the IBS-D cohort and HCs, indicating a significant difference in the MAM of the terminal ileum (Bray-Curtis-based and Jaccard-based ADONIS: P = 0.023, 0.002, respectively). The PCoA plots are shown in Figure 3d,e.
 Figure 3.:
Figure 3.: The alpha diversity and beta diversity analyses in patients with IBS-D and HCs. (a–c) The alpha diversity analyses in patients with IBS-D and HCs. Including Chao1, Observed species, and Shannon indexes. (d) Bray-Curtis–based PCoA plot in patients with IBS-D and HCs. (e) Jaccard-based PCoA plot in patients with IBS-D and HCs. *P < 0.05, **P < 0.01 compared with the HC group. HC, healthy control; IBS-D, diarrhea-predominant irritable bowel syndrome; PCoA, principal coordinate analysis.
Microbial compositionAt the phylum level, the mucosal microbiota of both groups was dominated by Firmicutes and Proteobacteria, followed by Actinobacteria and Bacteroidetes. The proportions of the dominant microbiota in IBS-D cohort were 60.18%, 17.57%, 13.06%, and 8.36%, respectively, whereas those in HCs were 35.92%, 47.74%, 9.69%, and 4.49%, respectively. At the genus level, the mucosal microbiota in the IBS-D group was dominated by Pseudomonas, followed by Shigella, Streptococcus, Collinsella, Ruminococcus, and Dorea. The proportions were 33.79%, 8.79%, 6.18%, 5.06%, 4.91%, and 4.21%, respectively. In the HC group, the mucosal microbiota was dominated by Ruminococcus and Streptococcus, followed by Pseudomonas, Collinsella, Faecalibacterium, and Bacteroides. The proportions were 11.88%, 10.26%, 8.05%, 7.37%, 6.92%, and 6.03%, respectively. The mucosal microbial composition of the terminal ileum in patients with IBS-D and HCs is shown in Figure 4a,b. What is more, differences in microbial composition between the two groups were identified through LEfSe analysis (Figure 4c,d). At the phylum level, the relative abundance of Proteobacteria (LDA score = 5.12, P = 0.001) was significantly elevated in patients with IBS-D compared with HCs, while that of Firmicutes (LDA score = 5.13, P = 0.003) was significantly decreased. At the genus level, the relative abundance of Pseudomonas (LDA score = 5.30, P = 0.035) and Lysobacter (LDA score = 4.03, P = 0.039) was significantly higher in the IBS-D group, while that of Bacteroides (LDA score = 4.26, P = 0.030), Ruminococcus (LDA score = 3.71, P = 0.008), Oscillospira (LDA score = 3.48, P = 0.035), Bilophila (LDA score = 3.64, P = 0.039), and Sutterella (LDA score = 4.32, P = 0.002) was significantly lower compared with HCs.
 Figure 4.:
Figure 4.: Mucosal microbial composition and LEfSe analysis in the terminal ileum of patients with IBS-D and HCs. (a) Relative abundance of mucosal microbiota at the phylum level in the IBS-D and HC groups. (b) Relative abundance of mucosal microbiota at the genus level in the IBS-D and HC groups. (c) Taxa enriched in the IBS-D group and HC group based on LEfSe analysis. (d) The cladogram showed enriched taxa in the IBS-D group and HC group based on LEfSe analysis. The English letters in the cladogram represent the taxa shown in the legend on the right. Only taxa with LDA scores > 2.0 and P values < 0.05 are presented. HC, healthy control; IBS-D, diarrhea-predominant irritable bowel syndrome; LDA, linear discriminant analysis; LEfSe, linear discriminant analysis effect size.
On further analysis for the secondary microbiome end point, we found that in the IBS-D with NLH group, patients displayed a significantly higher relative abundance of Proteobacteria phyla and Pseudomonas genera, while a significantly lower Firmicutes and Bacteriodetes phyla and Bacteroides and Oscillospira genera, compared with the IBS-D without NLH group and the HC group (Figure 5). These results suggested that the patients with IBS-D with NLH exhibited a more severe mucosal microbial disturbance of the terminal ileum.
 Figure 5.:
Figure 5.: Relative abundance of mucosal microbiota in the terminal ileum of patients with IBS-D with NLH, patients with IBS-D without NLH, and HCs. *P < 0.05, **P < 0.01 compared with the HC group. #P < 0.05, ##P < 0.01 compared with the IBS-D without NLH group. HC, healthy control; IBS-D, diarrhea-predominant irritable bowel syndrome; NLH, nodular lymphoid hyperplasia.
Correlation between mucosal microbiota and IBS-D symptomsWe further analyzed the correlation between the relative abundance of mucosal microbiota and the clinical parameters of VAS, DF, IBS-SSS, GAD-7, and PHQ-9 through the Spearman correlation analysis in the IBS-D cohort. The results showed that the relative abundance of Proteobacteria phyla was positively correlated with IBS-SSS scores (r = 0.44, P = 0.027) and the relative abundance of Pseudomonas genera was positively correlated with VAS scores (r = 0.45, P = 0.023) and IBS-SSS scores (r = 0.48, P = 0.014). Moreover, the relative abundance of Bacteroides genera was negatively correlated with IBS-SSS scores (r = −0.51, P = 0.009) and depression scores (r = −0.43, P = 0.031) while positively correlated with anxiety scores (r = 0.47, P = 0.017). The heatmap of the Spearman correlation analysis is shown in Figure 6.
 Figure 6.:
Figure 6.: Associations between the relative abundance of the mucosal microbiota in the terminal ileum and clinical parameters in patients with IBS-D based on the Spearman correlation analysis. *P < 0.05, **P < 0.01. DF, defecation frequency; GAD-7, generalized anxiety disorder questionnaire; IBS-SSS, IBS severity scoring system; PHQ-9, patient health questionnaire; VAS, visual analog scale.
DISCUSSIONAccumulating evidence suggests that gut microbiota, as important pathogenic factors, may lead to the pathogenesis of IBS-D (10–13). Most of the researches focus on the fecal microbiota, and the mucosal microbiota is not frequently studied in IBS-D. However, the intraluminal microbiota is very different from the mucosal microbiota; thus, it cannot completely reflect the microorganisms adhering to the mucosa (16). Moreover, the mucosal microbiota is closer to the host and more stable, which may be more relevant to clinical symptoms and deserves to explore (15,16). In this study, 16s rRNA sequencing for mucosal microbiota in the terminal ileum revealed altered microbial diversity and composition in patients with IBS-D, which may be associated with the severity of bowel symptoms.
Compared with healthy individuals, patients with IBS-D exhibited lower alpha diversity in the MAM of the terminal ileum, indicating a decreased mucosal microbial richness and evenness. Beta diversity also displayed a significant difference in the MAM of the terminal ileum between patients with IBS-D and HCs. These results are in lines with the changes of the fecal microbiota in some previous studies (25–27). For example, Phan et al (25) found that the fecal microbial alpha diversity was significantly lower in patients with IBS compared with that in HCs. Other studies revealed that the microbial richness was significantly decreased in the feces of patients with IBS-D, and lower microbial richness was associated with IBS symptom severity (26,27). Focusing on the mucosal microbiota, Matsumoto et al (15) found that the microbial evenness (but not richness) was significantly lower in the sigmoid colonic mucosa of patients with IBS-D than that in HCs. Based on these proofs, the microbial diversity of both fecal and mucosal microbiota may tend to be decreased in IBS-D cohort.
Moreover, we found that the mucosal microbiota in HCs was dominated by Firmicutes phyla (60.18%) and that in patients with IBS-D was Firmicutes (35.92%) and Proteobacteria phyla (47.74%). The relative abundance of Proteobacteria was significantly elevated while that of Firmicutes was significantly decreased in patients with IBS-D. At the genus level, the relative abundance of Pseudomonas and Lysobacter was significantly elevated in the IBS-D group, while that of Bacteroides, Ruminococcus, Oscillospira, Bilophila, and Sutterella was significantly decreased. Given that substantial evidence has underlined significant changes in Actinobacteria, Firmicutes, Bacteroidetes, and Proteobacteria phyla in IBS-D (10), our results are partially similar with the previous findings (11,12,27–30). Kerckhoffs et al (28) demonstrated that patients with IBS displayed elevated abundance of Pseudomonas aeruginosa, belonging to Pseudomonas genera, both in the feces and in the small intestinal mucosa. What is more, several studies have revealed a significantly lower abundance of Bacteroidetes phyla both in the feces and the mucosa of patients with IBS (10,11,29). In contradiction to that, there are some studies showing an elevated abundance of Bacteroides vulgatus and Bacteorides fragilis, both in the fecal and mucosal microbiota of patients with IBS (10,30). For Firmicutes phyla, contrary to our findings, some studies indicated an elevated relative abundance of Firmicutes in patients with IBS-D, especially Clostridia genera, both in the fecal and mucosal microbiota (10,12,27,29). Nevertheless, similar to our findings, patients with IBS-D exhibited a lower abundance of Ruminococcus and Oscillospira genera in the mucosa of the terminal ileum in a previous study (15). In addition, though some studies have demonstrated a significantly decreased abundance of Bifidobacterium genera in patients with IBS-D (10,12,27), we did not find an overt change in this study. In addition, microbial functional analysis was predicted by PICRUSt2 according to the Kyoto Encyclopedia of Genes and Genomes database. Predicted abundance of Kyoto Encyclopedia of Genes and Genomes functional pathways for all samples is shown in Supplementary Figure 1. Even if there was an overt change in microbial composition, we did not find significantly different metabolic pathways between the IBS-D group and the HC group. Collectively, our results suggested that the microbial diversity and composition in the mucosa of terminal ileum was altered, indicating a mucosal dysbiosis in IBS-D.
Of interest, we found that 40.0% of patients with IBS-D exhibited NLH on the mucosal surface of the terminal ileum, which indicated a low-grade mucosal inflammation. NLH is a benign overgrowth of lymphoid follicles, limited to the lamina propria and superficial submucosa layers of the intestine (31,32). Evidence has shown that patients with IBS are at higher risk of developing NLH within their intestinal mucosa (31). Commonly, NLH exists in the terminal ileum, but reported by a previous study, one-third of patients with IBS displayed NLH in the colonic mucosa (18,33). Although the pathogenesis of NLH is not fully understood, stimulation of intestinal allergens or pathogens might trigger the activation of mucosal inflammatory reactions and eventually develop NLH (33). Actually, it has been reported that gut microbiota plays an important role in the formation of NLH (20,33). In this study, compared with HCs and patients with IBS-D without NLH, patients with IBS-D with NLH displayed a more severe mucosal microbial disturbance in the terminal ileum. They showed a higher relative abundance of Proteobacteria phyla and Pseudomonas genera, a lower Firmicutes and Bacteriodetes phyla, and a lower Bacteroides and Oscillospira genera. These results are partially in line with the previous findings. Jiang et al (20) reported that the abundance of Bacteroides was significantly reduced in the MAM of the terminal ileum while the levels of some opportunistic pathogens (such as Haemophilus, Streptococcus, and Pseudomonas) were elevated in patients with NLH. Furthermore, Salarieh et al (18) found that the relative abundance of Bacteroidetes and Streptococcus was significantly lower in the mucosal microbiota of patients with IBS with NLH while that of Firmicutes, Pseudomonas, Haemophilus, and Campylobacter was significantly higher. In addition, a recent study from Chen et al has explored the relationship between mucosal inflammation and mucosal microbial dysbiosis. They found that the terminal ileum samples of children exhibited increased amounts of MAM and these adhesive bacteria (Clostridium, Veillonella, Ruminococcus, etc) induced the activation of Th17 cells and triggered secretory immunoglobulin responses (34). In this study, we suggested that mucosal microbial dysbiosis might be associated with the development of NLH in the IBS-D cohort, but we did not investigate whether the inflammation drove dysbiosis or vice versa. Longitudinal studies are still needed to explore the relationship between mucosal inflammation and microbiota dysbiosis.
Moreover, we explored the associations of the altered mucosal microbiota in the terminal ileum with bowel symptoms through the Spearman correlation analysis. The results showed that the relative abundance of Pseudomonas was positively correlated with abdominal pain and the severity of IBS, while the relative abundance of Bacteroides was negatively correlated with the severity of IBS. So we gave priority to these 2 bacterial species to speculate the underlying mechanisms. Pseudomonas is a kind of Gram-negative aerobic bacillus with flagella. In specific pathogenic conditions, it could produce several toxins (e.g., serine protease, lipopolysaccharide, and flagella), triggering the activation of mucosal inflammatory reactions and impaired mucosal barrier function, eventually leading to the symptoms of abdominal pain and diarrhea (10,17,35–39). Evidence has shown a high level of serine proteases in the supernatant of fecal samples from patients with IBS-D, and some special antibodies to flagellin (the main component of bacterial flagella) are found more often in patients with IBS compared with those in HCs (40–42). In addition, Bacteroides belongs to Gram-negative anaerobic bacillus, which can produce bile salt hydrolase, and participates in the biotransformation from primary BAs to secondary BAs (43). A growing body of evidence reveals elevated fecal BA levels and an increased proportion of primary BAs in patients with IBS-D, which is associated with bowel symptoms and disease severity (11,44–46). Therefore, the results of this study suggested that the mucosal microbiota dysbiosis in the terminal ileum (especially Pseudomonas and Bacteroides) might be associated with the development of IBS-D symptoms such as abdominal pain. However, longitudinal studies are still needed to establish causality between microbiota dysbiosis and the development of IBS-D symptoms.
Furthermore, we observed something confusing that Bacteroides was negatively correlated with depression but positively correlated with anxiety. To explain this, we reviewed several researches about the microbiome-gut-brain axis (47–53). According to a systematic review of gut microbiota and major depression disorder (MDD), the change of Bacteroides was divergent in 6 studies (47,48). Among them, Jiang et al (48) found that the patients with major depression disorder displayed a lower abundance of Bacteroides than that in HCs. In addition, some studies indicated that Bacteroides (such as Bacteroides fragilis) could produce large quantities of neurotransmitter γ-aminobutyric acid and patients with depression exhibited γ-aminobutyric acid deficits (49,50). Simultaneously, it has been validated that the relative abundance of fecal Bacteroides is negatively correlated with brain signatures related to depression (49). In addition, there are some studies focusing on the association between gut microbiota and anxiety disorders (51–53). Chen et al (51) found that fecal Bacteroides was more abundant in patients with active anxiety and positively associated with the severity of anxiety. Yang et al (52) reported that the abundance of mucosal colonic Bacteroides was positively associated with anxiety in patients with IBS-D. Based on these findings and our results of correlation analysis, we guess that the gut microbiota dysbiosis may contribute to neurotransmitter deficiency or enrichment through affecting amino acid metabolism, finally leading to psychological symptoms. However, possibly due to different anxiety and depression severity in patients with IBS-D and different metabolites produced by various bacterial species, the effects of microbiota on brain-gut axis are complex and need to be studied more accurately.
There are several limitations to our study. First, the sample size of this study is relatively small. Second, this is a cross-sectional, preliminary clinical study, which can only establish associations and not causality. Next, no positive or negative controls of the mucosal samples are set during the processing, quality control assessment, and sequencing. Furthermore, dietary variables in this study are not precisely controlled, and data on dietary questionnaires are lacking. Last, the colonic mucosal biopsies of the participants are not obtained. Altogether, longitudinal studies with larger-scale and well-matched cohorts are still needed to confirm the relationship between the mucosal inflammation, microbiota dysbiosis, and the development of IBS-D symptoms and to compare the mucosal microbiota of different regions of the gut in IBS-D.
In summary, this study demonstrated a dysbiosis of MAM in the terminal ileum in patients with IBS-D, and 40.0% of them exhibited mucosal NLH (a low-grade inflammation) with a more overt mucosal microbial disturbance. Furthermore, the alteration in mucosal microbiota may be associated with bowel and psychological symptoms. These results may provide new insights into the MAM and intervention of IBS-D.
CONFLICTS OF INTERESTGuarantor of the article: Sheng-Liang Chen, MD, PhD.
Specific author contributions: S.-L.C.: conceptualization. B.-Y.W., P.X., L.C., Q.-Q.W. H.-Y.Q., X.-J.Y., and S.-L.C.: data curation. X.-J.Y. and S.-L.C.: funding acquisition. S.-L.C.: validation. B.-Y.W. and P.X.: writing–original draft. S.-L.C.: writing–review & editing. All authors critically revised the manuscript and approved the final version of the manuscript.
Potential competing interests: The authors declare that they have no interest conflicts.
Financial support: The work was supported by National Natural Science Foundation of China (Grant No. 82170554 and 81970473 to S.-L.C., and 81970472 to X.-J.Y.).
Data availability statement: Data are available from the corresponding author on reasonable request.
Study Highlights
WHAT IS KNOWN ✓ Gut microbiota dysbiosis may contribute to the pathogenesis of diarrhea-predominant irritable bowel syndrome (IBS-D). ✓ The mucosa-associated microbiota (MAM) is rarely involved in IBS-D. WHAT IS NEW HERE ✓ Patients with IBS-D displayed a dysbiosis of MAM in the terminal ileum. ✓ The alteration of MAM in patients with IBS-D may be associated with bowel symptoms. ✓ Approximately 40.0% of patients with IBS-D displayed mucosal low-grade inflammation, with a more severe mucosal microbial disturbance. References 1. Longstreth GF, Thompson WG, Chey WD, et al. Functional bowel disorders. Gastroenterology 2006;130(5):1480–91. 2. Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: A meta-analysis. Clin Gastroenterol Hepatol 2012;10(7):712–21.e4. 3. Lacy BE, Moreau JC. Diarrhea-predominant irritable bowel syndrome: Diagnosis, etiology, and new treatment considerations. J Am Assoc Nurse Pract 2016;28(7):393–404. 4. Drossman DA, Hasler WL. Rome IV-functional GI disorders: Disorders of gut-brain interaction. Gastroenterology 2016;150(6):1257–61. 5. Saha L. Irritable bowel syndrome: Pathogenesis, diagnosis, treatment, and evidence-based medicine. World J Gastroenterol 2014;20(22):6759–73. 6. Zhan K, Zheng H, Li J, et al. Gut microbiota-bile acid crosstalk in diarrhea-irritable bowel syndrome. Biomed Res Int 2020;2020:3828249. 7. Rajilić-Stojanović M. Function of the microbiota. Best Pract Res Clin Gastroenterol 2013;27(1):5–16. 8. Canakis A, Haroon M, Weber HC. Irritable bowel syndrome and gut microbiota. Curr Opin Endocrinol Diabetes Obes 2020;27(1):28–35. 9. Martin CR, Osadchiy V, Kalani A, et al. The brain-gut-microbiome Axis. Cell Mol Gastroenterol Hepatol 2018;6(2):133–48. 10. Altomare A, Di Rosa C, Imperia E, et al. Diarrhea predominant-irritable bowel syndrome (IBS-D): Effects of different nutritional patterns on intestinal dysbiosis and symptoms. Nutrients 2021;13(5):1506. 11. Zh
Comments (0)