
Remember me
This systematic review protocol was developed in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) guidelines [24]. The systematic review will include reports of original research published in English and indexed in online databases up to February 28, 2023. Unpublished manuscripts, conference abstracts, case studies, case-series reports, and articles without full-text manuscript availability will not be included. Studies will be drawn from a wide array of online databases to cover the literature from multiple scientific disciplines. Searches will be conducted in Embase, PubMed, Cochrane Trials and Reviews, PsychInfo, and CINAHL. Additional papers will be identified by hand review of the included articles’ bibliographies.
Our focus will be on patients who received a diagnosis of hematologic malignancy between the ages of 15–39 years and subsequently underwent HSCT. Survivors of malignancies treated in childhood or in older adulthood will be excluded. Studies will only be included if data is stratified by age at cancer diagnosis or if the study is limited to AYA patients. Similarly, we are interested in recipients of HSCT for hematologic malignancies, so AYA patients who received HSCT for other indications (i.e., for breast cancer, testicular cancer, or benign hematologic conditions) will be excluded. As our research question focuses on long-term survivorship and the risk of death from acute complications of HSCT is highest in the first 100 days, we will exclude studies that only describe the effects during the first 100 days post-transplant [25]. Studies will be included if the outcomes reported incorporate at least one of the conceptual domains described above. Notably, we will include both positive and negative outcomes of HSCT, as both fit within the defined domains.
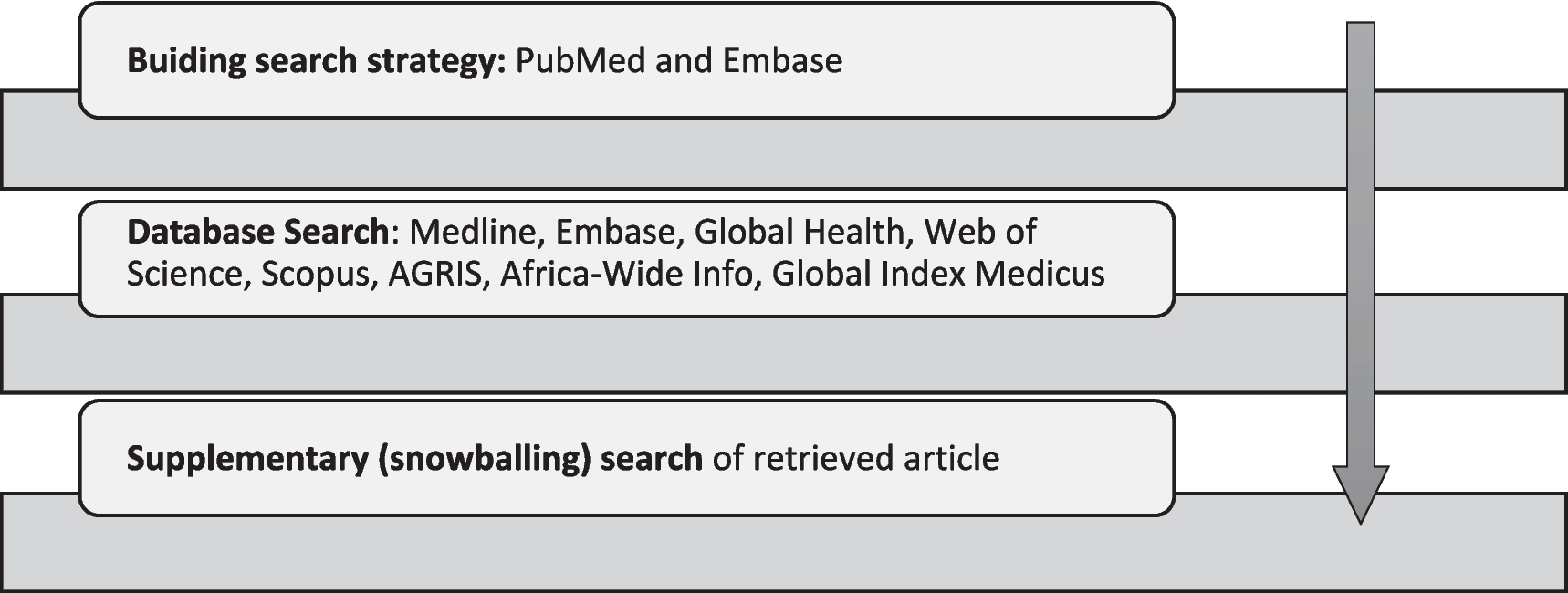
In collaboration with colleagues in the UCLA Louise M. Darling Biomedical Library, a finalized search strategy was developed based on the five survivorship domains and created to maximize both inclusivity and discernment around this unique research question. The final search strategy will encompass the concepts of “cancer” or “hematopoietic stem cell transplantation” and “adolescents and young adults” and “survivorship”. Please see Fig. 3 for an example of a complete search for PubMed. The search strategy will be translated as appropriate for all databases investigated.
Fig. 3
Search strategy. Example of literature search strategy for PubMed. Strategies for other databases were designed to reflect the content of the PubMed search
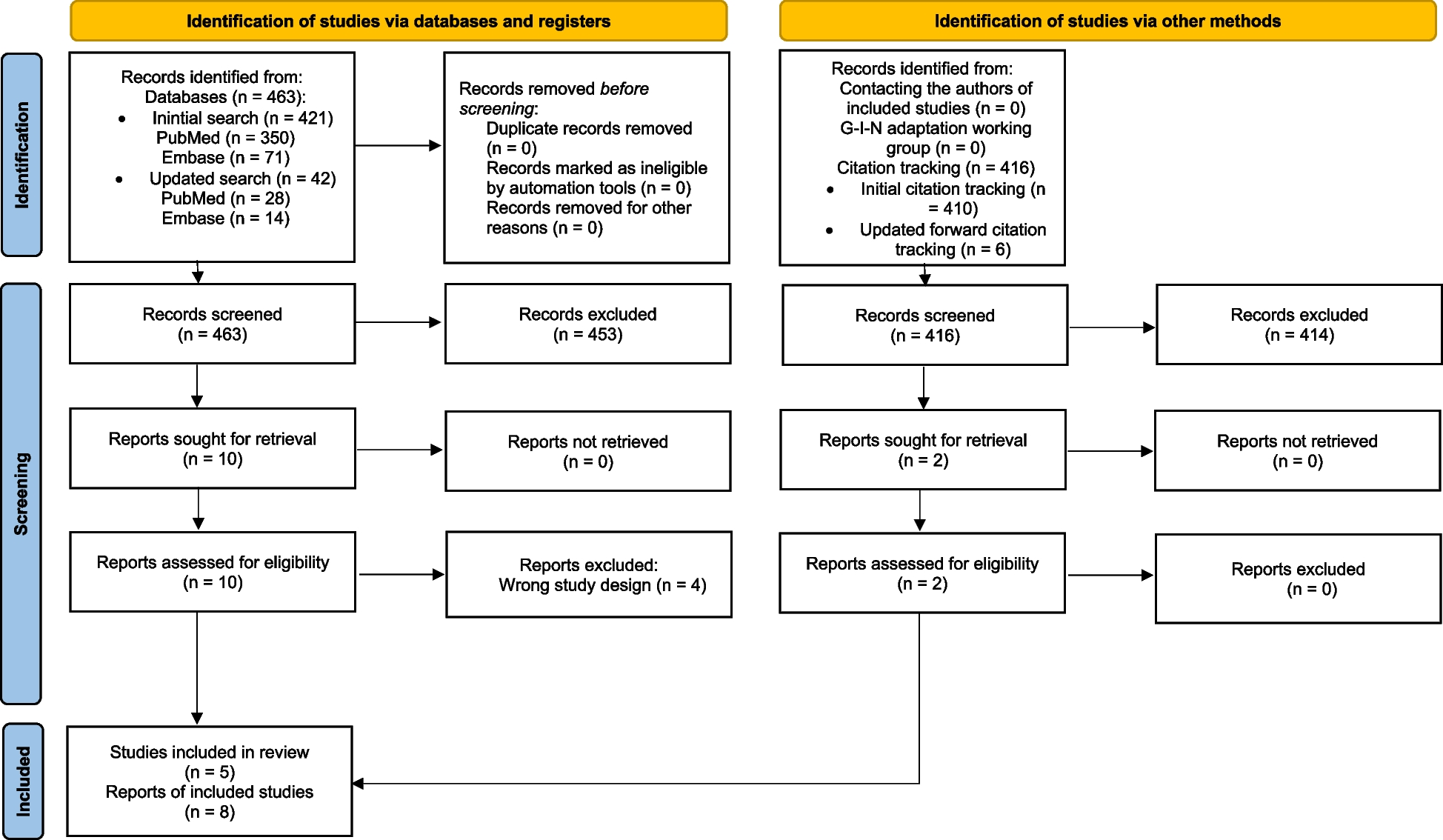
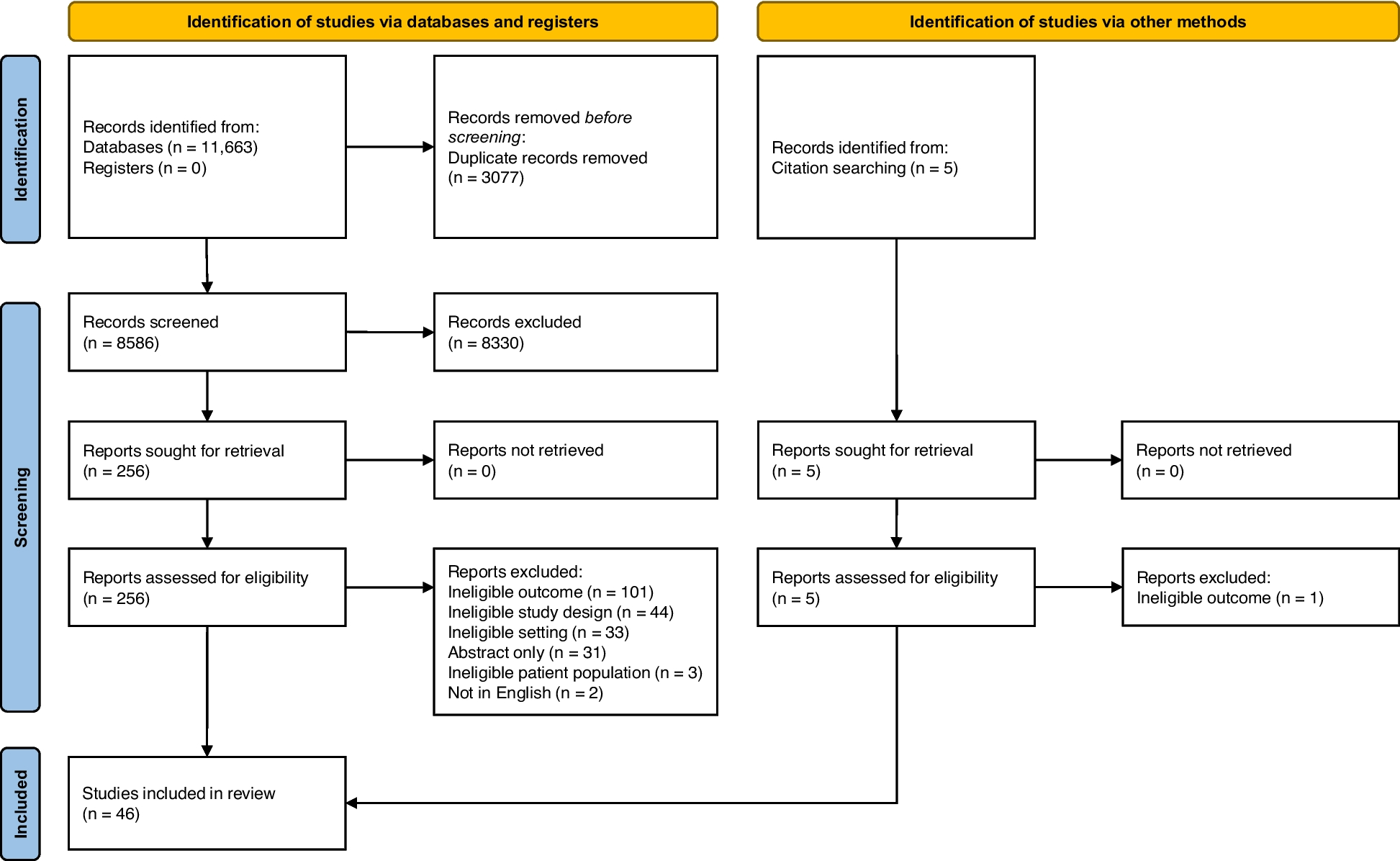
All search results will be managed using Rayyan Intelligent Systematic Review [26]. Search results from individual databases will be uploaded directly into Rayyan, and duplicates will be removed before screening. All screening decisions will be recorded according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (see Fig. 4). Screening of search results will commence with initial title/abstract screening by two independent, blinded reviewers. Regular reviewer meetings will be held, at first to identify points of clarification in screening protocols and then to discuss and settle any conflicting screening decisions. Inter-rater reliability will be calculated from the majority of screened articles, once the screening protocol has been tested and established. Any disagreements that cannot be resolved will be evaluated by a third reviewer. The decision rationale for each article reviewed will be documented.
Fig. 4
Proposed flow diagram. Derived from PRISMA 2020 flow diagram for new systematic reviews [27]
Articles that fail to be excluded by pre-determined criteria at this stage or articles for which more information is needed will move to a second, full-text screening stage. In the full-text stage, complete manuscripts will be attached to Rayyan entries for more in-depth review. Once again, two independent, blinded reviewers will conduct full-text screening according to established criteria. Inter-rater reliability will be calculated for the totality of full-text reviews. The decision rationale for each publication will again be documented. With regular meetings, we will attempt to reach a consensus should disagreement about inclusion arise. However, should consensus not be achieved, a third blinded reviewer will be incorporated.
Critical appraisal will then be assessed for each study included after full-text screening. University of Adelaide JBI Collaboration Critical Appraisal Tools will be used for critical appraisal and risk of bias assessment [28]. JBI tools were selected over others (such as ROBINS-I or CASP) primarily because we anticipate studies addressing this topic to be widely varied in study design and the JBI tools offer checklists tailored for different study structures. For each study, we will identify which checklist most appropriately reflects the design of the study and both reviewers will independently evaluate. Inter-rater reliability will be calculated. Studies will be included if > 70% of responses to checklist criteria are “yes”. If the two reviewers’ assessments are discordant, a third reviewer will assess. Should any study not have an appropriate checklist for risk of bias assessment using the JBI tools, it will be included to encompass as much of the literature as possible. Such articles will be marked as having not been assessed for bias.
Once articles for inclusion are finalized, data extraction will be performed independently by two reviewers. A detailed abstraction guide will be drafted, piloted, and adapted if needed to ensure standardized responses from all reviewers. Data will then be abstracted directly into a structured evidence table, with abstracted data blinded to other reviewers until the time of the joint review. Abstracted data will be jointly reviewed at regular intervals, and any discrepancies will be discussed until a resolution is reached. Data variables and outcomes to be abstracted are listed in Table 1. Given the nature of this review, outcomes will vary by article but will address at least one of the concepts included in the five domains of our conceptual framework (see Fig. 2). There will be no prioritization of outcomes as articles addressing any concept will be included in our qualitative review. Both first-order constructs (rates, distributions, proportions, direct study subject quotes) as well as second-order constructs (author interpretations, conclusions, or ideas) will be included as study outcomes.
Table 1 Data variables for extraction and their definitionsWhile data synthesis often involves both qualitative and quantitative analysis [29], we anticipate that the wide scope of this review will result in outcomes that cannot feasibly be quantitatively synthesized. Thus, we will focus primarily on qualitative synthesis. Data abstracted into evidence tables will be coalesced into summary tables by domain. In accordance with the Institute of Medicine standards for qualitative analysis [30], we will focus our synthesis on a descriptive review of the clinical and methodological characteristics of included studies, emphasizing strengths, limitations, and how bias could compromise the reported results. We will also identify patterns in findings across studies and examine how individual study characteristics impact these common themes and summative deductions. Meta-bias will be assessed across studies with attention to publication bias specifically. Finally, we will discuss the relevance of the included studies to our population of interest, identifying the gaps in the literature and opportunities for further study. Given the nature of the data, we will similarly forego formal assessment of confidence in cumulative data as tools such as the Grading of Recommendations Assessment, Development, and Evaluation (GRADE). Any major protocol amendments will be documented and resubmitted for review.
Comments (0)