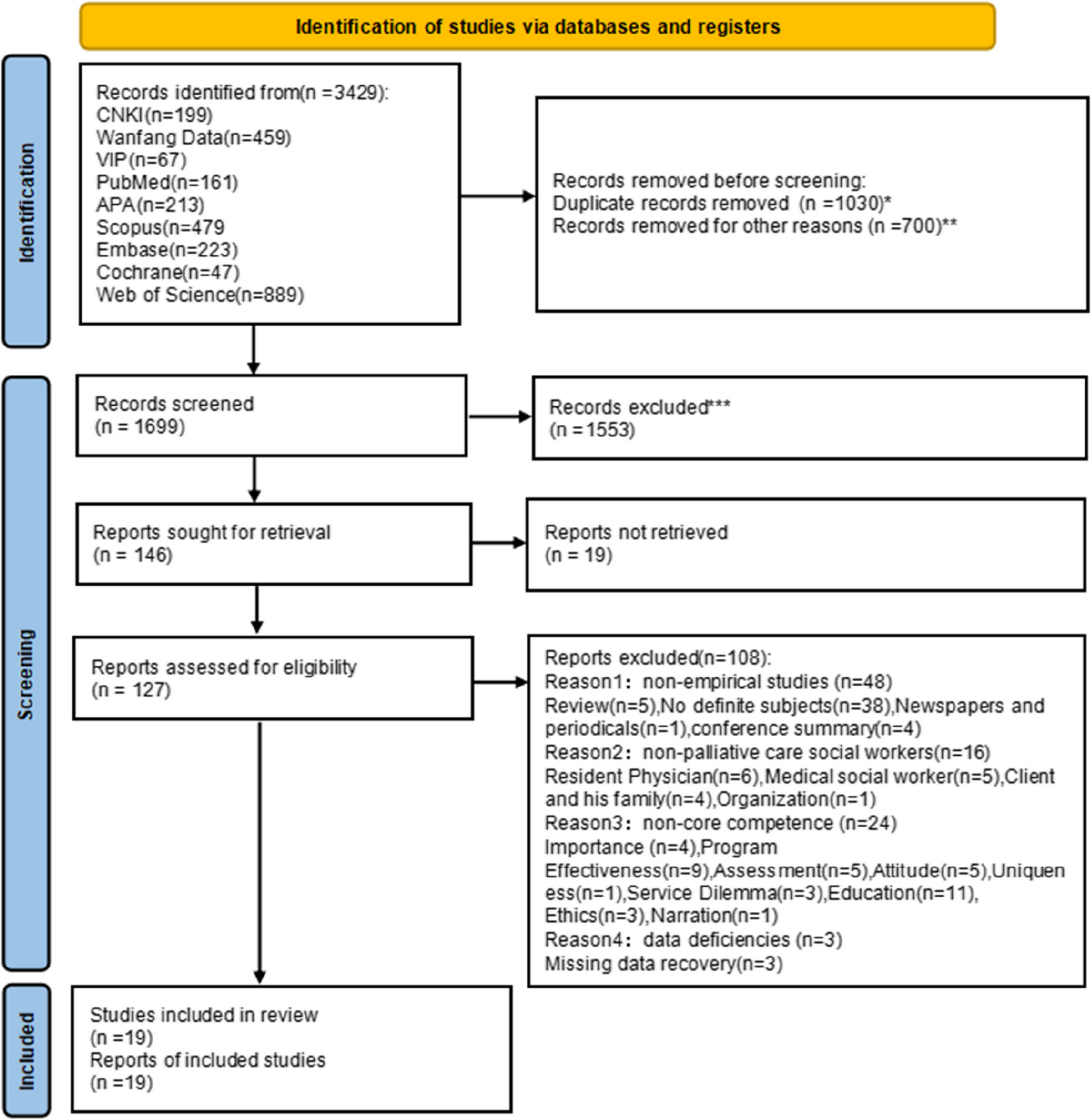
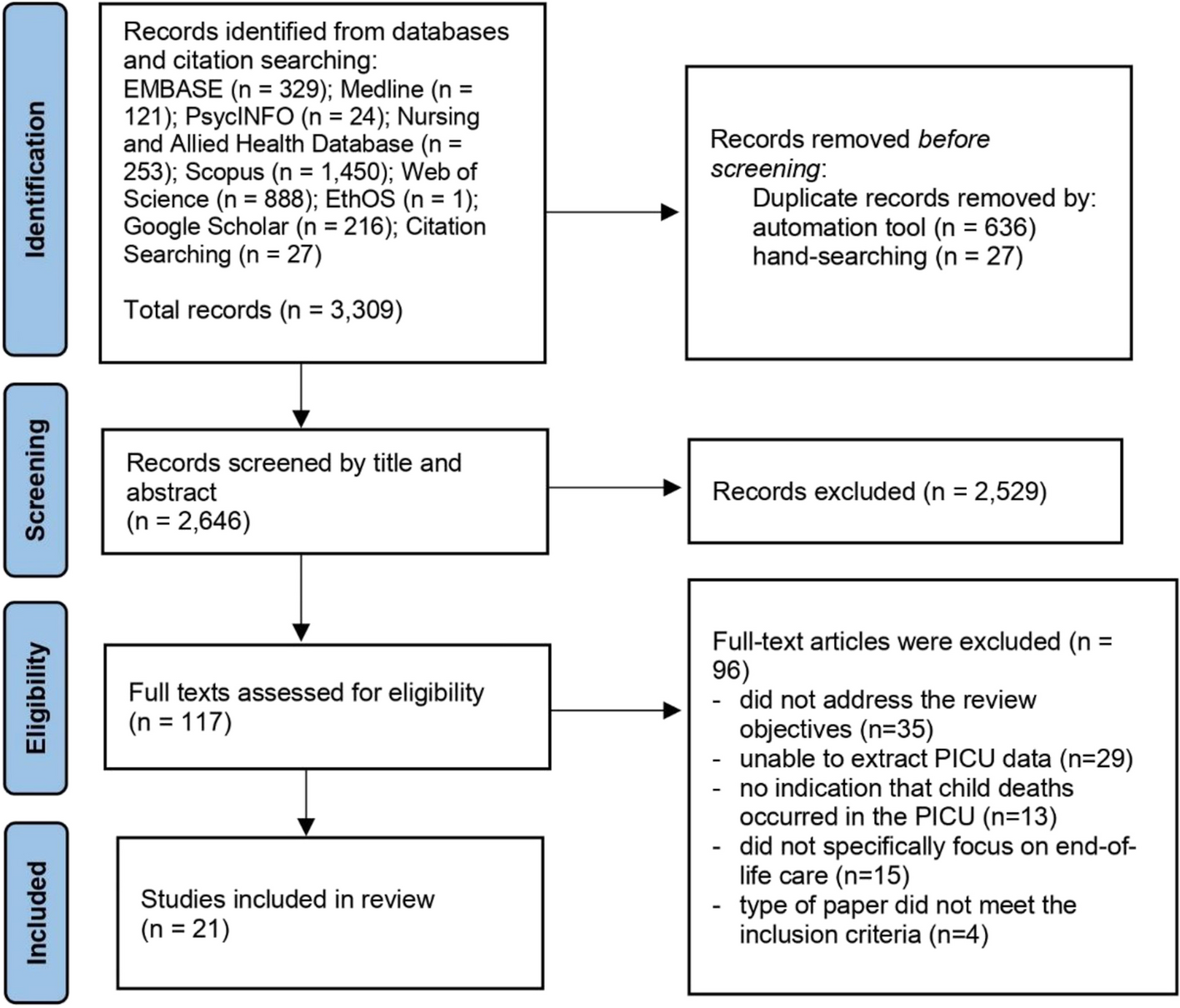
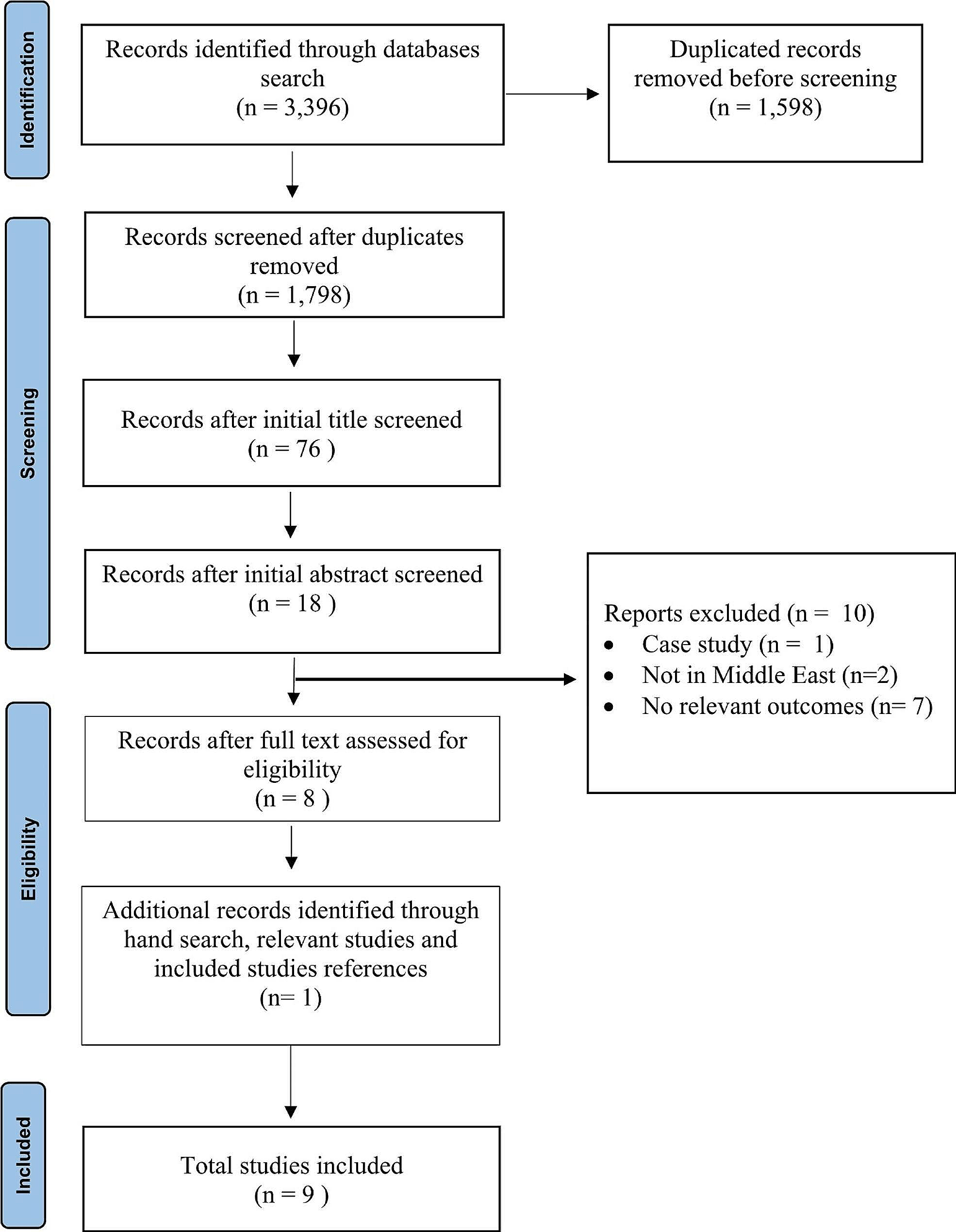
Across all searches a total of 7377 records were identified through database searching; 3393 duplicate records were removed, leaving 3984 records for title/abstract screening. After the title and abstract screening, 52 articles remained for full text screening of which 12 were eligible for inclusion in the review. Published between 2004 and 2021, the articles consisted of 1 review study, 10 research studies and 1 case study. Five themes and subthemes arose from the analysis consisting of: 1) valuing the whole person; 2) living while dying; 3) authentic death talk; 4) a supportive approach with the subthemes of presence and lack of support; and 5) a personalist approach. The results of the analysis of these studies are captured in the each of these themes and subthemes as laid out in this section.
Reporting of thematic analysis by themesTheme 1: Valuing the whole person
Valuing the whole person was thematically captured across the studies as the understanding that people are psychological, physical, and spiritual persons. The spiritual dimension of being human was particularly relevant across all populations under study. Parents of dying children expressed deep spiritual pain or a strong faith in relation to making meaning of their child’s suffering and death [20]. Parents also reported that a spiritual and moral struggle was necessary for some of them to find meaning in the experience of their dying child [24]. Some parents lost faith; for others it was reaffirmed [20, 24]. Dying children also wrestled with transcendental elements of dying and death; they described their anger toward spirituality or religion in relation to the suffering they were experiencing [22]. Conversely, spirituality was also captured as something that leant meaning to a child’s mortality, even in the midst of their dying [22]. Spirituality and spiritual care can also provide an opportunity for dying children to find meaning in life and suffering [25].
Children and their families reported that some healthcare professionals in hospice settings were able to address the psycho-spiritual dimensions of being a whole person [19, 28]. However, families also found that some healthcare professionals were uncomfortable with discussing spirituality; some healthcare professionals criticized families for considering morality and spirituality as relevant phenomena at the end of life [24]. Other healthcare professionals self-reported the relevance of spirituality as meaningful to the work they did with dying children [27].
Theme 2: Living while dying
The theme of living while dyingrevealed that living with a dying child can be all-consuming [24]. The ability for families to access healthcare professionals who have the perspective that dying is part of living alongside the necessary clinical skills to care for dying children is essential [18]. Such skills are a specialized area of care. Having the requisite outlook and skills creates meaningful opportunities for children, their families and carers to be transparent and open about healing, as well as personal and professional growth at the end of life. Utilizing palliative care principles positively emphasizes the life of the child as still living, and does not focus exclusively on their dying [18, 27]. Primary pediatric palliative care and SPPC are therefore relevant for seriously ill children because they support incorporating death into children’s perspectives on life as it is still being lived while allowing them to prepare for their end.
At the same time, living while dyingis challenging; parents caring for dying children still must live their own lives alongside their dying child. Having a dying child can be paradoxical for parents: knowing that their lives will continue after their child has died [22, 23]. For some siblings of dying children, death elicited fears of the unknown. Specifically, what would death be like for their dying sibling when it happened and for the sibling(s) left behind? [21] Siblings of dying children need support to process their grief after their sibling dies [21]. From the perspective of healthcare professionals, caring for dying children can be demanding, but it also provides time for healthcare professionals to reflect meaningfully on their work with dying children [27]. Children who are living while dying in the context of illness may endure pain and suffering [22]. Pain control and interventions to address the multifaceted dimensions of suffering are therefore necessary. However, suffering is not only pain oriented. Supporting dying children to find existential meaning, purpose, and hope amidst dying as part of living is also an essential facet of care for the child who is living while dying [25].
Theme 3: Authentic death talk
To support children in preparation for death as they live through the dying process, authentic death talk is crucial. However, talking about death is not a conversation that all parents feel comfortable or capable of having with their dying child [18, 26]. Some parents, siblings and families of dying children did not discuss the dying or death of a child at all. However, a lack of openness and authentic communication of the reality of what was happening led to some family members feeling “isolated” [21]. However, openly discussing dying and death in some instances brought cohesion, strength and a sense of support to families [21]. Similarly, dying children and youth want to talk about their dying and death and find such conversations important [22, 25, 26]. At times, authentic death talk needs to happen on behalf of children who are unable to speak for themselves. Such conversations require skilled, ethical consideration and respect for the need to protect children’s dignity in response to their increased dependency relative to their clinical and holistic care needs [29].
Theme 4 and subthemes: a supportive approach (lack or presence of support as subthemes)
Across the studies, the lack and presence of support for dying children are captured through the subthemes of presence and lack of support. The presence of support refers to families’ need for communities that will help them care for their dying children. Supportive clinical environments such as hospices, palliative care homes or units and bereavement programs can reinforce the importance of a specialized and appropriately contextualized healthcare environment when it is warranted for a child at their end of life [23].
Lack of support consists of healthcare professionals who showed a lack of appreciation or respect for the spiritual aspect of being human [24]. Similarly, expertise and training in SPPC as well as ethical preparedness for end-of-life care is lacking in Canada. Such expertise is necessary to provide excellent care to children who are dying [29] Lack of support also includes the dearth of practical resources. Some families reported that nothing in their dying child’s care trajectory was easily accessible: equipment, respite, interventions, and how to manage at home [24]. Families also remarked on the absence of community support in the context of Canadian healthcare. As Davies et al. found, “Traditional sources of family support such as extended families, churches and social organizations are no longer as prominent in our increasingly secular society” [18]. In response to the lack of holistic care and community connections, a supportive approach to care is needed in Canada that incorporates supportive sources of community into the care of dying children.
Theme 5: A personalist approach
Personalism takes the holistic aspects of being human into consideration through the lens of bioethics and by emphasizing the concept of interdependency [31]. While disagreements may arise between family and/or caregivers over what course of action should be taken in the dying child’s care, a personalist approach is needed, at times, to refocus such disagreements in an ethical light. For example, Gagnon and Kunyk identified that caregivers and families need to better differentiate when to transition dying children in pediatric intensive care units (PICUs) to SPPC [29]. In some instances, dying children in ICUs do not receive the SPPC they need because of interprofessional disagreements over when to transition them from active treatment to comfort care [29]. Gagnon and Kunyk point out that unresolved or prolonged disagreements can become an ethical concern for the dying child if it extends their suffering [29]. Moreover, Gagnon and Kunyk show that interprofessional disagreements may lead to healthcare professionals’ moral distress, which can manifest in inaction on behalf of the patients. Such inaction can be compounded by a lack of ethics expertise to navigate disagreements over complex care issues for dying children in PICU contexts. A personalist approach could be helpful in these situations because it necessitates moral engagement across disciplines, highlights interdisciplinary over disciplinary approaches to ethics, and accepts that healthcare occurs in light of interdependent relationships, which are essential in pediatric care.


Comments (0)