
Remember me



The scoping review search process initially resulted in finding 1644 documents through the 4 databases. Furthermore, 42 studies were also obtained through the Google Scholar. After duplicate removal, 1123 studies were identified for the title and abstract screening stage. Through this process, 976 irrelevant studies were removed, and the full-text reviewing process was initiated. Finally, 67 documents were also removed in this stage, as they did not fit the inclusion criteria or the objective of this review. Hand searching of reference lists led to 11 additional studies at the full-text review phase. This process led to the inclusion and analysis of a total of 80 studies presented in this scoping review. In Fig. 1, the results of searching, screening, eligibility, and inclusion processes have been demonstrated while applying the PRISMA methodology [22].
Fig. 1
PRISMA flowchart of the screening and review process for included studies
The synthesis process led to categorizing the included studies into three categories (1) Clinical population studies, (2) Workers’ population studies conditions, and (3) General wearable design/performance studies. The summarized results for each category are presented in the following. Tables 1, 2, 3 provide the extracted detailed information of included studies in each category.
Table 1 Clinical population studiesTable 2 Workers’ population studiesTable 3 General wearable design/performance studiesAmong the identified body of evidence, various researchers from 30 countries have contributed to this field by conducting studies. In Fig. 2, the number of conducted studies in each country has been demonstrated in a bar chart. Researchers of the USA, Canada, Italy, China, and Germany are pioneers in this field by presenting 18, 12, 7, 6, and 6 studies, respectively. It must be noted that in the case of collaborations of researchers from different countries, all author’s affiliations have been considered the origin country of research.
Fig. 2
Number of included studies sorted by the countries
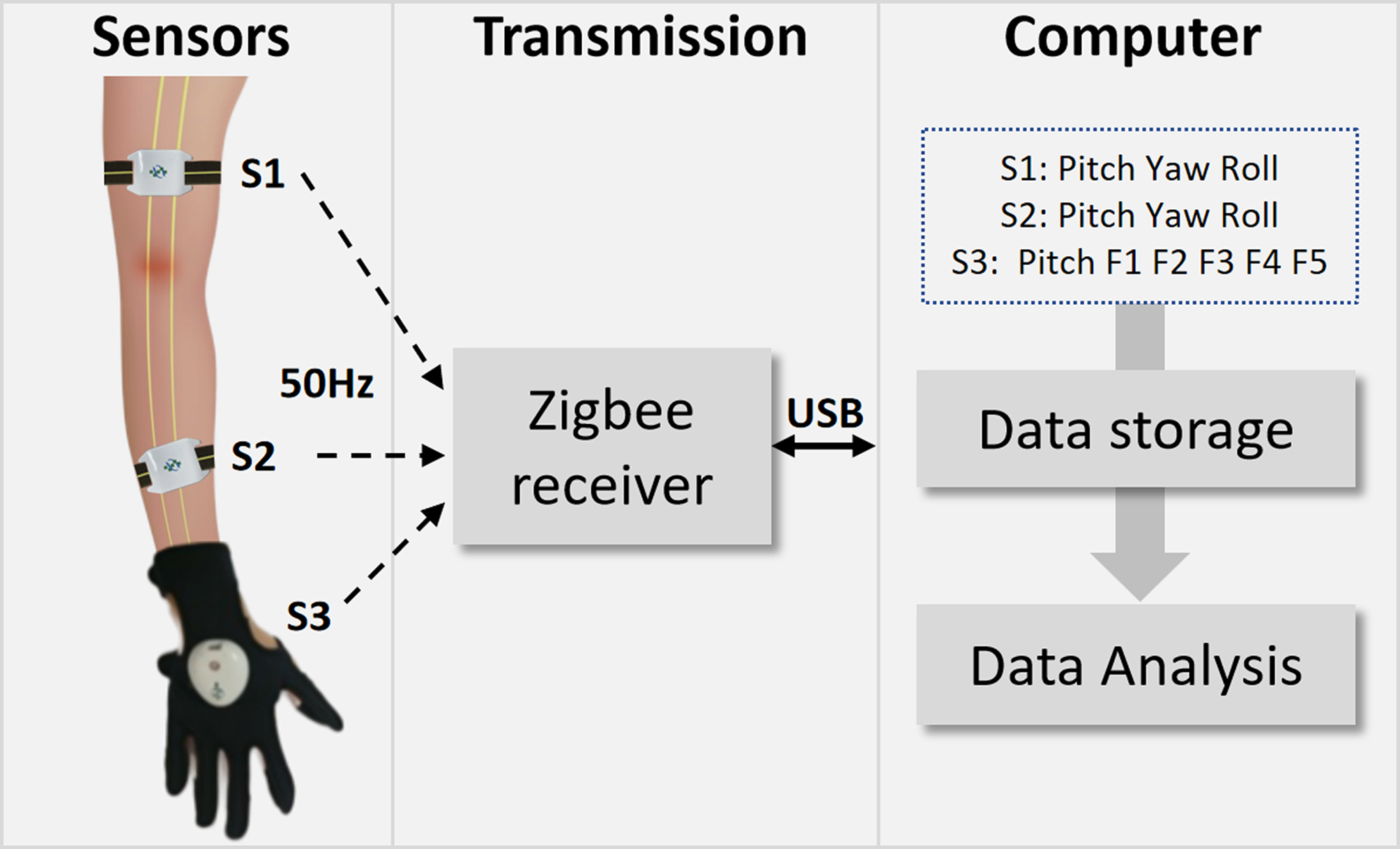
The sensor placement locations were sorted into (1) shoulder and upper arm (scapula and humerus), (2) elbow, forearm (ulna and radius), and wrist and (3) hand, and finger (phalanges). (Fig. 3) Most of the included studies (n = 76) have attempted to measure angles of these limbs (for obtaining Range of Motion or ROM) alongside their angular velocity or acceleration through exploiting IMU, piezoresistive, or optical sensors providing three-dimensional values (represented in Quaternion axes, Eulerian axes, or yaw/pitch/roll). In these studies, subjects performed a series of various joint movements such as flexion/extension, abduction/adduction, and internal/external rotation or a combination of these motions to obtain the measurement parameters of that joint. A summary of the data collection procedures along with the critical points regarding the processing methods used for the translation of obtained joint data into meaningful clinical or non-clinical outcomes have been reported for all three categories in Additional file 2: Appendix B.
Fig. 3
a Sensor placements at different segments for all included studies; b Sensor placements at different segments in clinical population, workers’ population, and general design/performance studies, separately
The outcome column of the following tables summarizing the extracted data of included studies presents the corresponding outcome that has been directly or indirectly obtained via wearable sensor platform. If the targeted outcome of a study is indirectly measured by the wearable sensor platform, the sensor-measured parameters (joint angle, acceleration, or angular velocity) are mentioned in brackets. Moreover, if the outcome obtained by wearable sensors is a secondary outcome of the study, it is demonstrated in that section. Since the assessment and collection of the statistical results of the studies are outside the scope of this scoping review, the related information about the statistical processes and analyses has not been reviewed. We also presented an overall visual representation of the total number of various sensor types used in all the studies, utilizing a pie chart (Fig. 4).
Fig. 4
Number of different types of sensors used in all studies; Examples of others include smartwatches, self-developed systems, LED, and non-IMUs
Clinical population studiesIn this category, either the participants of the included study were MSK patients, or the introduced wearable platform was designed and aimed to be applied to individuals with MSK conditions. A total of 31 articles were identified to be included in this category. Nineteen studies out of 31 were related to applications of wearable sensors for shoulder or upper arm conditions. However, the sensor placement of some of these studies included other upper body parts such as the wrist [24,25,26,27,28] and hand [29]. One of the included studies has utilized a wrist wearable system for assessment purposes on patients with distal radius fractures [30]. Three other studies on arthritis and motor impairment patients have used wrist-mounted wearable sensors [31,32,33]. Five studies focused on hand and finger diseases such as hand arthritis [34, 35] and carpal tunnel syndrome [36, 37], applied wearable sensors (such as IMUs, and piezoresistive sensors) that were either embedded in a glove or attached with straps.
The study design types of included articles in this category were case–control studies (12 studies), case series studies (13 studies), and preliminary studies (6 studies), without any Randomized Clinical Trials (RCT) studies (Fig. 5).
Fig. 5
Study design types of included articles in the clinical population studies category
Most of the studies (n = 26, 84% of clinical population studies) exploited IMU sensors in their wearable platform (usually containing a 3-axis accelerometer, 3-axis gyroscope, and 3-axis magnetometer) to obtain joint angles, accelerations, angular velocities, and posture. While only five studies have included EMG sensors in their wearable platform to obtain muscle activity [30, 38,39,40,41]. Some of the studies have also used other instruments and sensors to obtain measurements or treat an MSK condition, such as using high-power LEDs [42] and thermal flexible printed circuit boards for treatment [32] or using piezoresistive or strain sensors for measurements [35,36,37, 43]. In the sensor type and hardware column of Table 1, the model and provider company of sensor, the attachment or embedding method of the sensor in wearable platform, core processing unit, and data sampling frequency of wearable sensors were indicated (in case of reporting by authors).
In the included studies, participants completed functional activities or exercises, like shoulder flexion/extension, abduction/adduction, and internal/external rotation, or wrist, elbow, and fingers flexion/extension for a specific set of repetitions in standardized conditions such as in studies conducted by Duc et al. [38], Kwak et al. [24], and Chen et al. [44]. Some studies have collected the data in a non-standardized set up like a home setting. In these studies, participants’ daily activities have been recorded and analyzed, such as in studies conducted by Pichonnaz et al. [45], Duc et al. [46], Van de Klut et al. [47], Langohr et al. [48], and Haverstock et al. [49]. The explained wearable systems have been identified as home-based wearable systems and have been reported in Table 1. It must be noted that usually, the calibration process of sensors has been described, and a summary of these procedures has been included in Additional file 2: Appendix-B (in case of reporting by authors).
The software utilized for each study’s processing phase (translating raw data into the intended outcomes) has been indicated in the “Software for processing/data display” column of Table 1.Each study’s home-based applicability, comfortability assessment, and wireless data transmission ability have been examined in the final column. In this regard, the introduced wearable system of 17 studies (55% of this category’s studies) has been recognized as home-based applications. Only 1 study (3% of this category’s studies) have assessed the comfortability of their applied wearable sensor platform in subjects [25], and 10 studies (32% of this category’s studies) have explicitly mentioned the ability to send the measured data through a wireless system [25,26,27, 29, 33, 35, 37, 39, 40]. This ability is a crucial parameter for the future development of wearable systems. The share of each sensor placement location in the studies has been demonstrated (Fig. 6).
Fig. 6
Sensor placements at different upper limb segments for Clinical population studies category
Workers’ population studiesIn this category, 31 studies have focused on the workers’ population and the risk of work-related musculoskeletal (WMSK) conditions or disorders. Two RCT studies, a crossover study, two case–control studies, 21 case series studies, and 5 preliminary studies are included in this category (Fig. 7).
Fig. 7
Study design types of included articles in the Workers’ population studies category
From the perspective of sensor placement location, 21 Studies (68% of studies in workers’ population category) have placed the sensors on multiple arm segments (the most common segments are the upper arm and shoulder). This can indicate that the most studies of this category have correctly assessed more than one single-point arm segment to obtain a complete perspective of the risk involved in various working conditions. It can be deduced that the primary focus point of these studies is upper arm segment (Fig. 8).
Fig. 8
Sensor placements at different upper limb segments for the Workers’ population studies category
The participants of this category’s studies form diverse samples of different populations including, dentists [55,56,57], surgeons [58, 59], warehouse and manufacturing workers [60,61,62], farmers [63, 64], athletes [65], and other areas. According to Table 2, nearly all the studies have either aimed to investigate ergonomic risk levels of a specific job or measure the exposure to ergonomic risks related to WMSK conditions. A significant number of the studies (about 48% of the included studies) have exploited Rapid Upper Limb Assessment (RULA) score (or a modified version of it), which represents the level of MSD risk for a job task being evaluated [66]. Thus, the RULA score is one of the frequently reported outcomes of a considerable number of included studies of this category. Some of the studies have aimed to evaluate the validity of a proposed wearable sensor platform for monitoring the ergonomic performance of workers with respect to an optical motion capture system accepted as a gold standard [67,68,69].
Regarding the utilized instruments and hardware of wearable sensors applied in the studies, IMU sensors have been exploited in all studies. In this regard, seven studies have declared that Xsens company (headquartered in the Netherlands) products, including MVN link and Biomech™, were used to obtain inertial measurements [55,56,57, 63, 67,68,69]. It can be implicated that due to convenient application, and various provided features, Xsens products are more favorable for researchers aiming to study work-related musculoskeletal risks or non-laboratory setup and locations. Six studies have also utilized sEMG recording electrodes in their system to obtain muscle activity of arm segments [63, 64, 69,70,71,72]. One study has included force sensors in addition to embedded IMU sensors in a glove to acquire complementary information regarding the work-related ergonomic risks of hands and fingers [73].
Two studies have devised a haptic feedback system via a vibration actuation unit in their wearable system design to provide alerts for workers for changing their posture [62,
Comments (0)