
Remember me
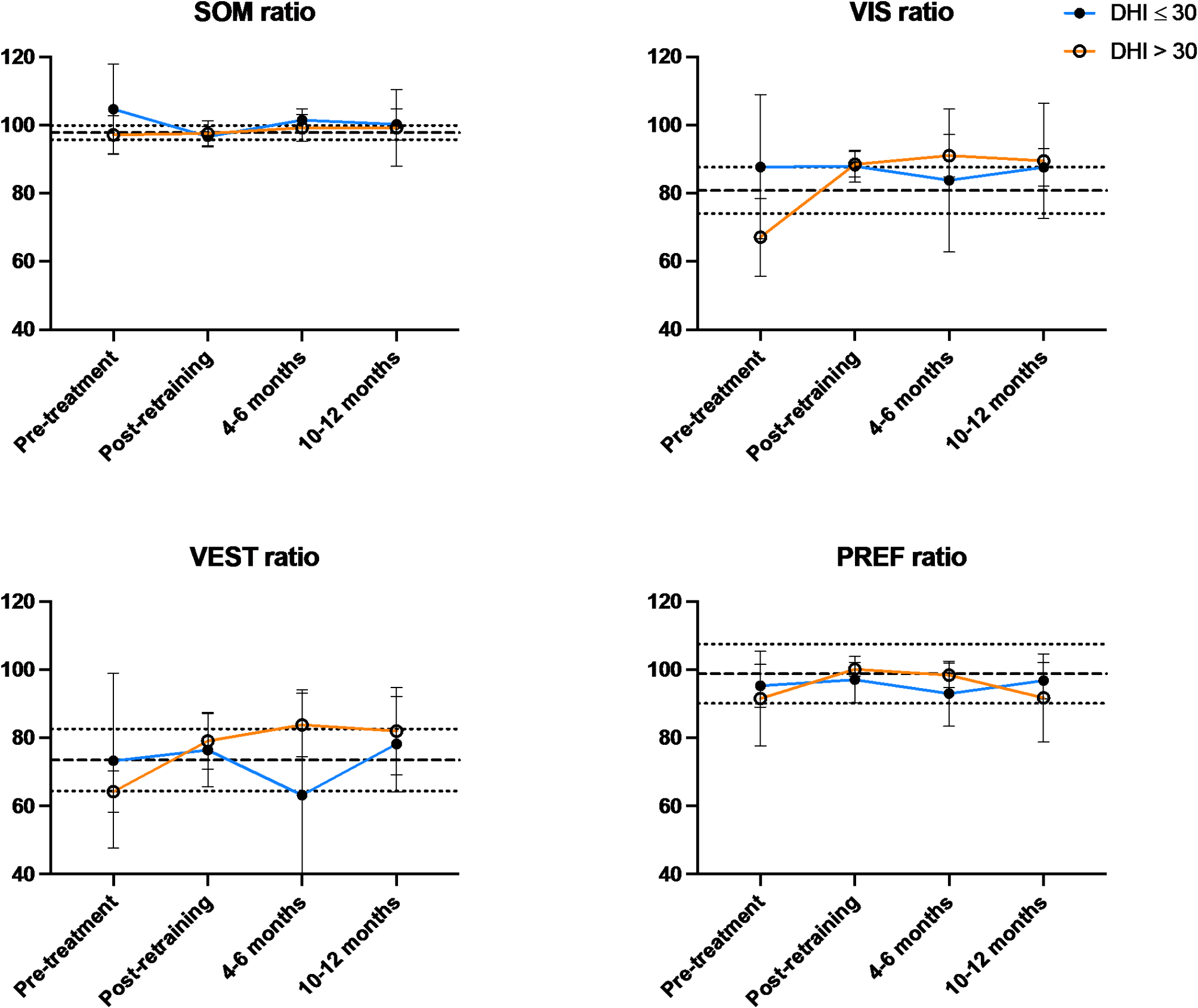



This study used the SOT test, an objective posturography assessment, to measure changes after CVRT in postural control of patients with symptoms lasting greater than 6 months. The participants in this study had stable symptoms for greater than six months and had achieved static compensation; accordingly, they all had SOM ratios near 1. The VIS and VEST ratios both incorporate testing on the sway-referenced platform, which presents a significant challenge to postural control. Indeed, balance scores on the sway referenced platform were significantly lower than on the fixed platform, both for healthy participants [22] and for those with vestibular deficits [19]. After CVRT, participants displayed improved postural stability on the sway referenced platform, both in the presence of visual cues (VIS) and in their absence (VEST). There was no change in PREF, suggesting no strong visual dependence (Table 3; Fig. 2). Collectively, these changes associated with CVRT, independent of visual cues, suggest that improved postural stability arose from a gain in vestibular function.
Fig. 2
SOT sensory ratios at baseline, immediately post-retraining, and at 4–6 months and 10–12 months after retraining. Asterisks indicate improvement compared to baseline (P < 0.05). The heavy dashed line is the normative mean and the light dotted lines are +/- one SD from the mean.1
In the days after unilateral vestibular injury, the asymmetry in neural activity of the vestibular nuclei is modulated to restore homeostasis. This coincides with acute compensation, whereby spontaneous nystagmus is resolved and static balance symptoms are greatly ameliorated. Improvements in dynamic balance, through complex and diverse electrophysiologic and behavioral changes, continue to take place for most individuals over the ensuing weeks; however, many individuals continue to experience significant morbidity months or years after onset, even with treatment [6].
Horak found that well-compensated patients had lower vestibulo-ocular reflex gains than poorly compensated patients and suggested that residual, possibly distorted vestibular information was worse than none at all; however, those who learned to use remaining vestibular information from the intact ear performed better than those who relied heavily on visual and somatosensory cues [12]. Individuals with vestibular deficits may adopt diverse motor learning strategies navigate the requirements of daily life [23] and these strategies may place a higher or lower dependence on vision [24].
Consistent with this literature, we observed significant inter-individual variability in our participants prior to CVRT. The changes we observed after CVRT, namely improved global balance performance even in the absence of a somatosensory reference and of visual cues, coupled with the reduction in the between-participant variability, suggest that that compensation by use of remaining vestibular function, as described by Horak, was taking place for the participants in this study.
Vestibular rehabilitation modalitiesOne consequence of continuous and evolving compensation is that early compensatory changes take place while neurological healing and restructuring is ongoing. Tighilet and Chabbert wondered, in their 2019 review, how sensory input from re-afferentiated vestibular organs would be re-integrated and whether repaired synapses that do not exactly recapitulate the pre-injury state could lead to aberrant sensory input during movement [2]. For some patients, early compensation strategies that are ‘good enough’ may fail to reintegrate retained or restored vestibular function into their postural maintenance strategy. Training protocols that call upon vestibular input may promote reweighting from an over-reliance on vision and somatosensation to a more balanced integration of sensory information that makes use of vestibular senses retained by the patient. However, common treatment modalities may not elicit such balanced compensatory responses [11, 25].
Most rehabilitation modalities seek to recalibrate postural (and ocular) control to habituate to vestibular information that is absent, corrupted, or asymmetric. Through coordinated head, body, and eye movements, patients are trained to cope with their vestibular deficit and maintain postural control primarily through the visual and somatosensory cues [12].
Virtual reality-based interventions have attracted the attention of researchers and clinicians; however, there is conflicting evidence concerning whether such interventions are superior to conventional vestibular exercises [26,27,28,29]. Many of these interventions were designed as more engaging alternatives to conventional vestibular exercises [27, 30]; however, most share with conventional exercises that they are designed to promote habituation and adaptation by encouraging head and eye movements in conjunction with concordant visual information. It is less clear that these types of exercises help with dynamic balance and improve capacity to manage discordant sensory information; indeed, some forms of visual stimuli may even exacerbate visual dependence [11].
There is some evidence in the literature that training that incorporates incongruent sensory information– that is, when visual, somatosensory, and vestibular cues are not in agreement– may help improve dynamic balance. For instance, training using tilting platforms [10, 31] prompts patients to maintain their balance in a dynamic environment in which somatosensory input from their feet and ankles in unreliable.
Compensation achieved through suppression of vestibular information, as occurs in the acute phase of vestibular injury and as evidenced by atrophy of parts of the brain involved in vestibular processing [32, 33], may limit the potential for dynamic recovery when vestibular loss is partial or temporary. CVRT seeks to train patients to use their remaining vestibular function, either in conjunction with congruent visual and somatosensory information, or to overcome incongruent visual and somatosensory cues, in a manner that more closely replicates the integration of sensation by individuals with no deficit. By challenging participants to maintain their balance on an unsteady surface and in visually complex environments, participants in this study improved their postural control in in a variety of conditions.
The capacity of the vestibular system– both central and peripheral components– to change, regenerate, and repair, help to explain the mechanisms by which many individuals recover high levels of function after vestibular loss. Such research also offers insight on how individuals that do not achieve robust dynamic compensation, either spontaneously or through standard vestibular therapy, may benefit from retraining. In this pilot study, CVRT was associated with improved postural control consistent with increased weighting of information from the vestibular organs– either on the unaffected side or from intact organs on the affected side– over vision through a mechanism of vestibular plasticity.
Comments (0)