This study illustrates a variety of postnatal growth patterns for preterm infants in a LMIC setting who received KMC in early life. Certain birth and early life factors were associated with different growth patterns, and certain growth patterns may be useful for identifying infants at risk of underweight, stunting, wasting and overweight at 1 year. This could have clinical utility for flagging infants at risk of adverse growth outcomes, facilitating timely support and appropriate intervention.
For each anthropometric indicator, over 80% of the infants fell within the healthy age-corrected z-score range of -2 to +2 at 1 year of age, where one would expect ~95% of the children in an optimally nourished population to fall. The relatively high rates of excess underweight, stunting and wasting (above the expected ~2.3%) in the sample are not unexpected, given the well-described risks of sub optimal growth outcomes in SGA and preterm infants [1,2,3]. Furthermore, catch-up growth is likely to be incomplete at 1 year of age, and can reasonably be expected to continue through the second year of life; thus, the rates of underweight and stunting may well decrease further over time. In a large Canadian study that followed early preterm infants (GA 24–29 weeks) up to 3 years CA, the numbers of infants with WAZ or LAZ < -2 decreased progressively from 4 to 36 months CA [21], although the study included a much smaller proportion of SGA infants (4.9%) than our sample (32.0%). The substantial catch-up growth in our study sample is further illustrated by the fact that the rate of stunting, at 17.0%, is substantially lower than the reported South African population prevalence of stunting (31.4% in infants 12–17 months old) [22]. Taken together, this provides support for early, prolonged KMC, strong breastfeeding support and regular infant follow-up as strategies to optimise preterm infant growth in a resource-constrained LMIC setting.
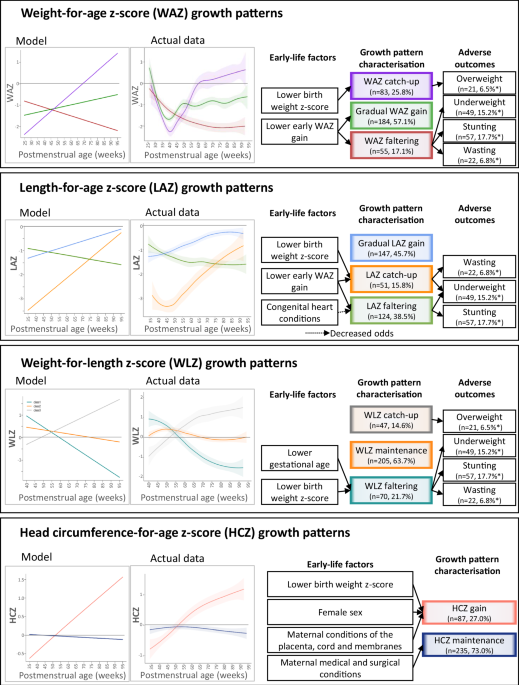
Over 80% of infants were classified as having acceptable WAZ growth patterns (i.e. gradual WAZ gain (184/322, 57.1%) or WAZ catch-up (83/322, 25.8%)). While the gradual WAZ gain pattern did not reach BWZ, the plateau level was above the lowest WAZ, possibly reflecting physiologic postnatal weight loss and regain. Consistent with research showing that few preterm infants regain their BWZ by 40 weeks PMA [23,24,25,26], the gradual WAZ gain and WAZ catch-up growth patterns only started increasing after term age. Guidelines for preterm infant growth targets recommend at least maintaining the WAZ at which weight gain starts, even if the BWZ is not regained [23,24,25,26]. More than 60% of the infants had appropriate LAZ growth (i.e. gradual LAZ gain (147/322, 45.7%) or LAZ catch-up (51/322, 15.8%)), yet a considerable number exhibited LAZ faltering (124/322, 38.5%). Preterm infants with insufficient LAZ catch-up growth are likely to remain stunted throughout childhood. With an estimated preterm birth rate of 13% ( ~ 150,000 preterm births annually) [27], LAZ faltering in preterm infants is of particular concern as a possible contributor to childhood stunting, which remains prevalent in South Africa [22]. For WLZ, the majority of the infants displayed a WLZ maintenance pattern (205/322, 63.7%), with a further 47/322 (14.6%) attaining WLZ catch-up, which may be considered a more appropriate growth pattern in this sample due to the large proportion of SGA neonates. The 47 infants (14.6%) who displayed WLZ faltering are a group of concern, particularly given the strong association between WLZ faltering and wasting at 1 year in this sample. Though most infants exhibited acceptable growth and anthropometric status at 1 year, it is important for the clinician to be cognisant of growth patterns that may indicate an increased risk of malnutrition. In this regard, infants with WAZ, LAZ and WLZ faltering represent the groups of highest concern for undernutrition at 1 year (Table 4). Identifying the early-life factors that are associated with these growth patterns may therefore be useful in flagging infants whose growth should be monitored more closely.
Of the early-life predictors, BWZ and early WAZ gain (up to 50 weeks PMA) were most consistently associated with 1-year growth patterns. Lower BWZ was associated with WAZ and LAZ catch-up, consistent with literature describing higher postnatal growth velocity in SGA infants compared to AGA infants [7, 28, 29]. In this sample, SGA infants had considerably smaller WAZ gains up to 50 weeks PMA (−0.36 ± 1.22 vs. 0.04 ± 1.08 z-scores, Supplementary Table 1), in contrast to other research showing greater early growth in SGA infants [29]. However, SGA infants did have greater overall WAZ gain in the first year of life (0.47 ± 1.20 vs. 0.08 ± 1.31 z-scores, Supplementary Table 1). In the context of lower BWZ following intrauterine growth faltering due to placental insufficiency [30,31,32,33], adequate postnatal nutrition can result in accelerated growth and return to the genetic growth potential [23]. Conversely, lower BWZ was also associated with WLZ faltering, raising the possibility that WLZ faltering may co-exist with seemingly adequate WAZ and/ or LAZ growth. Literature has long described sub-optimal long-term growth outcomes in SGA infants [1,2,3, 5, 34,35,36]. In univariate analyses, SGA performed similarly to BWZ, but associations became non-significant when SGA and BWZ were both included in multiple regression analysis. This may imply that BWZ predicts growth patterns even in non-SGA infants, particularly since WAZ and LAZ faltering were associated with higher rather than lower BWZ. Our results furthermore suggest that, despite the more rapid postnatal WAZ and LAZ growth experienced by smaller infants, catch-up growth was still incomplete at 1 year, and disproportionate WAZ and LAZ growth may still result in WLZ faltering. This further emphasises the importance of longitudinal WLZ growth monitoring, and argues against SGA as an isolated indicator of malnutrition risk.
Smaller early WAZ gains (up to 50 weeks PMA) were associated with WAZ faltering, slow WAZ growth, LAZ faltering and LAZ catch-up, while the greatest early WAZ growth was associated with WAZ catch-up and gradual LAZ gain. The associations between early WAZ growth and WAZ patterns are not surprising since one is a subset of the other. The relationship between WAZ and LAZ growth patterns is less well established, though one Bangladeshi study found that stunting at 12 and 24 months was predicted by earlier episodes of weight faltering [37]. The WAZ and LAZ catch-up growth patterns were associated in the lowest rates of underweight, wasting and stunting, but the highest rates of overweight. This has been observed in previous studies, where early growth was protective against undernutrition, but excessive early weight gain was associated with later overweight [38]. Research in various LMICs likewise identified failure to regain birth weight by two weeks of age (indicating insufficient early growth) as a risk factor for stunting and underweight at 6 months old in term and preterm low birth weight infants [34].
Lower birth GA was associated with WLZ faltering, which was in turn associated with higher rates of underweight, stunting and wasting. Preterm birth is a well-established risk factor for long-term growth deficits, particularly when complicated by SGA [1,2,3,4, 6].
Infant congenital heart conditions were only associated with LAZ growth patterns, with an increased odds of LAZ catch-up and decreased odds of LAZ faltering (compared to gradual LAZ gain). Though congenital heart conditions were also associated with WLZ faltering in univariate analysis, the association became non-significant in multivariable analysis, suggesting that this association may be mediated by lower GA or lower BWZ (both of which were associated with congenital heart conditions in this sample). Congenital heart conditions are more often associated with sub-optimal growth outcomes, and in this sample the infants with congenital heart conditions were smaller at 1 year. However, they also had lower birth weight z-scores and gestational age at birth, which emerged as significant predictors of WAZ and WLZ growth patterns in multivariate analysis, while congenital heart conditions did not. This may be attributed to the fact that the congenital heart conditions observed in the sample were mostly associated with delayed adaptation to preterm birth (PDA, 65/100 cases and patent foramen ovale PFO, 47/100 cases), and in all but one case resolved early in the neonatal course, either spontaneously or with the administration of non-steroidal anti-inflammatory drugs. Minor cardiac defects like PDA and PFO are often associated with preterm birth; thus, it is reassuring to know that in this sample of infants they were not associated with sub-optimal postnatal growth patterns. Ventricular/ atrial septum defects (present in eight infants in this sample) are potentially more problematic, and deserve investigation in a larger sample.
The lack of a distinct HCZ faltering growth pattern is reassuring, as HC growth predicts neurodevelopmental outcomes in preterm infants [39, 40]. Our research did not assess neurodevelopment, but HCZ growth pattern was not associated with 1-year malnutrition.
To the best of our knowledge, this is the first study to use LCTM to characterise longitudinal WAZ, LAZ, WLZ and HCZ growth patterns in South African preterm infants. This research is potentially useful in clinical practice, facilitating the identification of particularly nutritionally at-risk preterm infants by characterising early-life risk factors and growth patterns associated with adverse growth outcomes. However, the study sample cannot be considered representative of all South African preterm infants, as it was limited to a small geographic area, and included a larger-than-typical proportion of SGA infants. The sample size was also insufficient to allow for detailed investigation of the association of infant comorbidities with growth patterns, particularly for less prevalent conditions. Moreover, routine clinical data has some inherent limitations, particularly regarding the completeness of maternal health information. The lack of reliable birth length and HC measurements is another important limitation that should be addressed in future research and clinical practice. Finally, while not all infants require catch-up growth, for those who do, 1 year was likely insufficient to capture the full extent of catch-up growth, which may be expected to continue up to 2 years of age. This is particularly apparent in the LAZ catch-up growth pattern, which still had a steep upward slope by the end of the study period. Likewise, capturing the development of overweight/obesity in this population will require longer follow-up.
Many questions remain for future research. At the most basic level, a clear definition of appropriate early catch-up growth remains elusive, as any definition of catch-up growth would have to consider the selection of growth indices to consider, the magnitude of the z-score gain, and the time over which the growth took place. Due to the computational complexity, machine learning and automated pattern recognition methods may be useful to assist in delineating the limits of appropriate growth versus growth faltering in relation to key outcomes. The role of infant feeding practices and dietary intake deserve special attention, not only as predictors of growth but also as potential interventions to promote more favourable growth trajectories. Body composition assessment would also be valuable, since it is known that preterm infants tend to have lower fat-free mass and higher fat mass percentage than term-infants at term-equivalent age [25]. Knowing how body composition evolves throughout childhood and beyond would offer important insights into the metabolic risks associated with different growth patterns.


Comments (0)