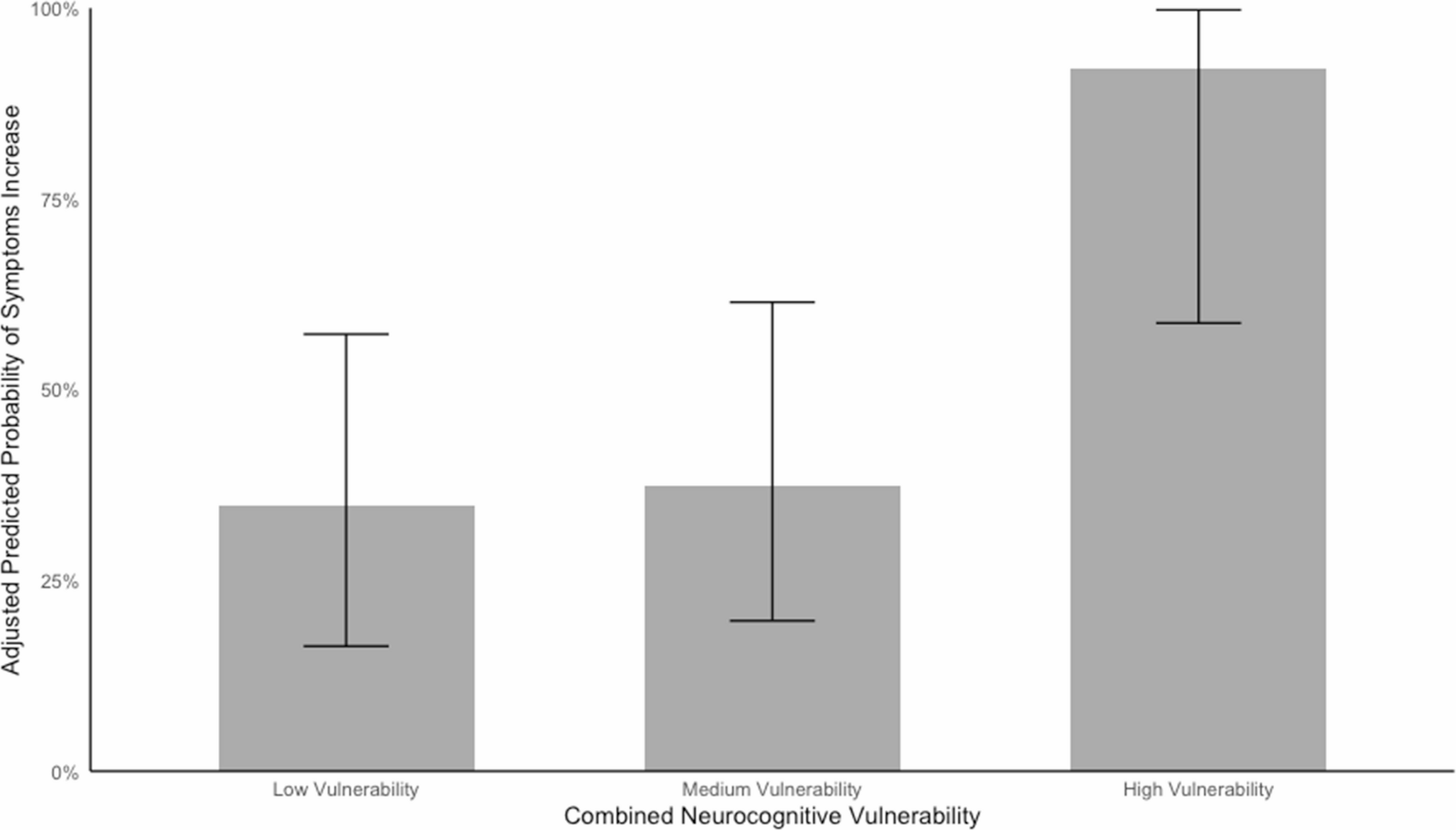
In the context of increased emphasis on mental health prevention, the aim of the current longitudinal study was to examine whether a range of neurocognitive probes could be used to detect psychiatric vulnerability among maltreatment-exposed children. There were two main results. First, we found that a combined neurocognitive vulnerability metric, spanning various domains of social cognition and reward processing, predicted future symptom increases in maltreatment-exposed children. Even after controlling for baseline symptoms and clinical status, children classified as high-vulnerability (i.e. with atypical functioning in two or three neurocognitive domains) were substantially more likely to present with worsening mental health symptoms at follow-up 1.5 years later. Second, children with maltreatment exposure, compared to propensity-score matched non-maltreated peers, had higher combined neurocognitive vulnerability scores. That is, they were more likely to exhibit atypical neurocognitive functioning across multiple domains.
Building upon prior efforts, this study introduces a fresh approach for assessing latent psychiatric risk in maltreatment-exposed children, before frank psychopathology has emerged. Prior research that has sought to identify those who may be most vulnerable predominantly focused on the severity of maltreatment, such as the number of adverse childhood experiences [14, 15], isolated neurocognitive domains [34,35,36], or aggregate indices of demographic, intellectual functioning, and psychosocial risk [9]. As we move more towards a model of secondary prevention the timely identification of children at increased psychiatric vulnerability is essential to ensure support and intervention during this critical period – before symptoms emerge, become ingrained, and are thus harder to treat. We know that maltreatment-exposed individuals who develop mental health problems often have a poorer prognosis and can respond less favourably to treatments [37,38,39]. Therefore, accurate early identification is both an ethical and economic necessity [8]. Our preliminary findings suggest that integrating neurocognitive probes across multiple domains offers a promising avenue for adding clinically meaningful information to individualised risk assessments. This approach may also help identify possible aetiological mechanisms that could be prioritised in any preventative intervention aimed at fostering resilient outcomes.
Another key novel contribution of this study is that a cumulative measure, encompassing multiple domains of neurocognitive functioning, may be feasible and effective for detecting maltreatment-related recalibrations. This is consistent with the view that maltreatment experiences result in system-level neurocognitive alterations across multiple domains [5, 20]. Crucially, the group difference in the neurocognitive vulnerability metric was independent of potentially confounding demographic or cognitive factors that were stringently controlled for using PSM. This finding, while requiring replication, highlights the potential for three important lines of future enquiry. First, indexing a constellation of concurrent domains in future research may help identify which neurocognitive subdomains are more strongly associated with specific outcomes (e.g., internalising vs. externalising symptom clusters, difficulties in educational settings, poor interpersonal functioning). Second, this multiple-domain approach may also motivate new research that can contribute to current debates about how different dimensions of childhood maltreatment – such as the developmental timing of exposure [40, 41], subjective appraisal of early trauma [42], and types or number of early adverse events [43, 44] – may contribute to specific neurobiological and psychological outcomes. Third, and perhaps most tentatively, our findings raise the possibility that it may not be the degree of atypicality within any single neurocognitive domain that best signals psychiatric vulnerability, but rather the accumulation of alterations across multiple domains. In this sample, children exhibiting atypical performance in more than two domains were at greatest risk of symptom increases over time. While replication is needed, this cumulative pattern may reflect system-level disruptions with functional consequences that are not easily captured when focusing on isolated constructs. Future work should therefore examine whether multi-domain profiles outperform dimensional scores from any one task, and explore the potential existence of a latent neurocognitive risk factor using larger samples and multivariate analytic approaches. This should include comparisons with more conventional aggregation methods, such as z-score-based composites or weighted continuous scores.
Given the preliminary nature of this study, several important limitations must be acknowledged when interpreting the results and planning future research. First, we examined a limited range of neurocognitive domains. This study should be expanded to include additional domains associated with maltreatment exposure and known to be potential mechanisms of latent vulnerability [5, 24, 45]. We would suggest that this should encompass, but not be limited to: executive functions critical for effective interpersonal interactions, such as emotional regulation; interpersonal problem-solving delay discounting; and declarative memory, including autobiographical memory. Second, the current sample size limited our ability to employ more complex multivariate analytic approaches, such as confirmatory factor analysis and machine learning techniques. This limitation is particularly relevant for the high-vulnerability subgroup, which included a relatively small number of participants, and therefore findings relating to this category should be interpreted with caution. These methods, facilitated by a large sample, could provide more fine-grained insights into the existence of the proposed ‘latent’ theoretical construct (i.e., maltreatment-related cumulative neurocognitive vulnerability) and help identify the most relevant and potent predictors of psychiatric vulnerability.
Third, while our use of a binary outcome (symptom increase vs. stable/decrease) aligns with the study’s preventative aims, we acknowledge that this approach does not capture the magnitude or clinical meaningfulness of symptom change. Our primary goal was to identify children who may be on a worsening trajectory — before symptom escalation reaches diagnostic thresholds. However, this method has limitations. Symptom change was operationalised using caregiver-reported SDQ scores, which may not fully capture difficulties across all domains or do so equally across groups, particularly when caregivers differ in their relationship to the child (e.g., parent vs. professional carer). Future studies should therefore incorporate multiple-informant assessment approaches to improve the robustness and comparability of outcome measurement. Additionally, longer follow-up intervals and more frequent symptom assessments would enable testing whether cumulative neurocognitive vulnerability also predicts the onset of diagnosable psychiatric disorders or more substantial clinical deterioration. Such extensions would help clarify the prognostic value of this metric across different stages of vulnerability and disorder emergence. We also recognise that future studies should formally compare modelling strategies — such as treating neurocognitive predictors and symptom change as continuous versus categorical — to determine which approach most effectively captures cumulative neurocognitive vulnerability and its clinical relevance. Finally, there is growing recognition that the impact of maltreatment-related neurocognitive recalibrations in shaping future outcomes is modulated by domains of interpersonal functioning, such as the presence of adaptive or maladaptive support networks, social competence and confidence [6]. Identifying such social factors in future research could be leveraged to increase the translational relevance of these findings, directly informing the development of evidence-based preventative interventions that could foster adaptive interpersonal functioning. Fourth, follow-up data were available for only a subset of participants, due to study design constraints. Nonetheless, comparisons across baseline characteristics revealed no strong or systematic differences between participants with and without follow-up, suggesting that attrition is unlikely to have introduced substantial bias (see Supplementary Table S2).
Despite these limitations, this study has several notable strengths. First, it is the first to apply a combined neurocognitive vulnerability metric in a maltreatment-exposed sample, offering a novel experimental approach to predicting psychiatric vulnerability in this high-risk population. By focusing on prediction, the study provides a valuable tool for identifying children most at risk for future mental health problems. Second, the recruitment of a sample with substantiated maltreatment exposure adds robustness to the findings, ensuring that the observed relationships are grounded in well-documented cases of adversity. Finally, the longitudinal design enables the tracking of changes in symptoms over time, providing a more comprehensive and nuanced view of risk trajectories compared to most neurocognitive studies of childhood maltreatment, which typically employ a cross-sectional design.
In conclusion, this study introduces a novel cumulative neurocognitive vulnerability index that simultaneously captures alterations across multiple domains of neurocognitive functioning. The results suggest that this assessment method may hold significant implications for prevention science, particularly in identifying children at heightened psychiatric risk following maltreatment exposure. Developing cost-effective screening tools is a crucial stepping stone, as these tools are necessary for determining who should be prioritised when deploying indicated preventative approaches. Only by accurately identifying those at greatest vulnerability can we design affordable, scalable approaches that effectively offset risk trajectories and reduce the mental health impact of childhood maltreatment.


Comments (0)