4.1. Significance of the study
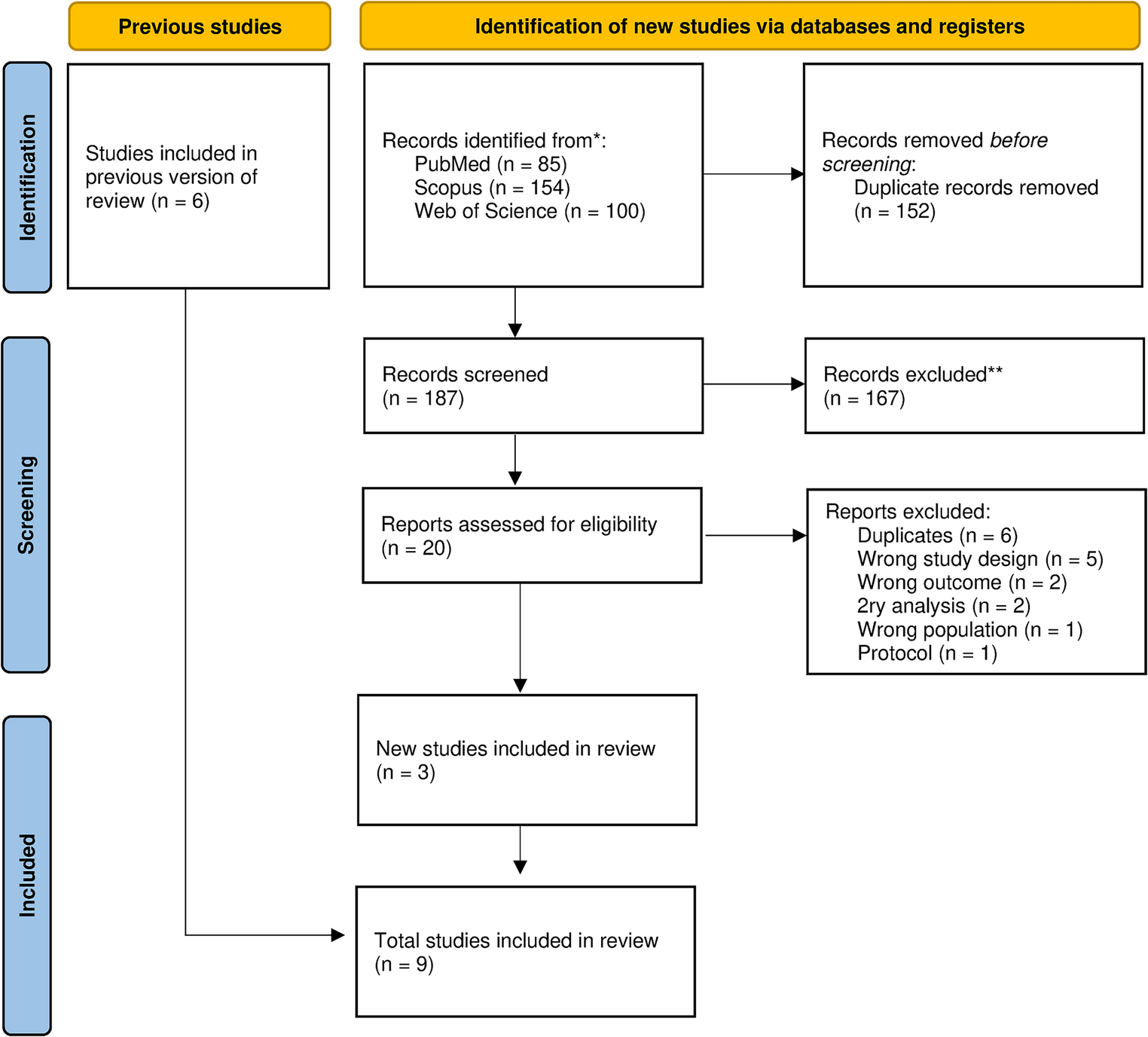
This updated meta-analysis reassessed bumetanide’s efficacy and safety in treating children with ASD by including three additional recent RCTs with larger sample sizes and longer treatment durations [8, 18]. This addition raised the total to nine eligible RCTs involving 920 participants, which is almost double the sample size of the previous meta-analysis. Additionally, two of those recent studies are large phase III multicenter trials that failed to show significant differences between the bumetanide and placebo groups [8]. These conflicting results with the previous meta-analysis mean that adding such studies to the pooled evidence is essential to obtain better insights on the efficacy of Bumetanide in ASD.
4.2. Summary of the findings
Our pooled analysis showed a significant difference between the bumetanide and placebo groups in the Childhood Autism Rating Scale (CARS), favoring the bumetanide group. Our pooled mean difference did not reach the − 4.5 point of minimal clinically important difference [19]. Moreover, both studies conducted by Du et al. and Lemonnier 2012 et al., with no significant heterogeneity, found that bumetanide led to a statistically significant improvement in the Clinical Global Impressions-Efficacy Index (CGI-EI) [13, 14]. On the other hand, bumetanide has no significant effect on reducing RRB after using different tools, including ADOS RRB, SRS-2 RRB, ABC RRB, and RBS-R. Moreover, no differences were observed in other outcomes, such as the Social Responsiveness Scale (SRS-2), Social Interaction and Communication (SI), and Sensory Affection.
The results of Shaker et al. were always more significant and did not overlap with the other studies. However, sensitivity analysis showed that its removal only eliminates heterogeneity without affecting the overall significance. This means that the significance of our results was not driven by a single study.
The main side effects were polyuria and hypokalemia, which, despite causing more withdrawals in the bumetanide group, were managed with dietary adjustments and potassium supplements. Other serious side effects were rare and probably unrelated to the treatment.
4.3. Explanation of the findings
Bumetanide is a loop diuretic and selective inhibitor of the Na-K-Cl cotransporter (NKCC1). It can improve ASD symptoms by reducing the intraneuronal chloride and transforming excitatory GABAergic signaling into inhibitory. This restores the GABAergic excitatory-inhibitory balance, which is thought to be the main contributor to ASD symptoms [6, 20] (mollajani, Zhang 2020). Our meta-analysis showed a significant change in CARS score in favor of the bumetanide group. This could be explained by the reduced GABA/Glx ratio in the insular cortex, which is believed to be responsible for sensory integration, emotional and autonomic signals, cognitive resources allocation, and behavior control [21]. Our finding was consistent with most of the included studies except for Fuentes A and B studies, where the CARS score declined post-intervention but did not reach statistical significance. This could be due to the higher baseline symptom severity of the patients included in these trials. Moreover, there was a relatively higher placebo response in these trials, which could be explained by natural fluctuations in the disease course leading to regression of symptom severity after a peak severity that was present at inclusion. Another possible explanation is that in these trials, unlike similar clinical trials, the included patients were allowed to take additional psychotropic medications, which could interfere with the accuracy of the results [8]. It’s worth noting that these studies were of a high risk of bias, which could've resulted in bias in the outcome assessment. On the other hand, among the trials that reported consistent results to our meta-analysis, Dai et al. included children below 7 years, which could lead to more favorable outcomes due to the rapid brain development and the highest rate of social and cognitive development [17]. Additionally, in Du et al., the intervention used was a combination of bumetanide and applied behavior analysis (ABA). This combination therapy was suggested to provide better results due to the biological cellular stability achieved by bumetanide, which was hypothesized to pave the way for a better brain susceptibility to ABA [14].
When conducting subgroup analysis to assess different factors that might affect the bumetanide response, we found that a significant effect of bumetanide was observed only after 3 months. There is a debate that 3 months is too short to detect treatment effect. Early trials suggested clinical signs of response, but investigators consistently urged additional research with longer duration. However, the recent phase III study (Fuentes at al.) that extended to 6 months over a large sample size failed to replicate the positive findings from earlier trials [8]. Qualitative exit interviews indicated some perceived improvement at week 26, such as emotional calmness and interaction, which may not have been fully captured by standard scales used in the trial [22]. This discrepancy could be driven by the difference in the phase of included trials. Moreover, it could be due to the nature of the treatment being symptomatic, not curative. It is worth noting that the 6-month subgroup only included 3 studies, which is too small to detect significance. Additionally, two of these studies [8] had a high placebo response, which might contribute to the overall non-significant results.
Regarding the SRS-2 scale, two out of three clinical trials reported a significant difference in favor of bumetanide. However, our pooled analysis showed non-significant differences. This could be due to the small number of trials reporting this outcome. Additionally, in Sprengers 2021 which showed non-superiority of bumetanide, there was a high placebo effect, which could be the reason why they failed to detect statistical significance [16]. This could be due to the inclusion of older children (>7 years), unlike the other two trials, which included younger age groups [15, 17].
The conflicting results among different scales could be due to the lack of standardization regarding the tool used to assess the treatment effect in ASD trials. Multiple clinical trials used CARS as the primary outcome measure. However, CARS is generally used as a screening tool for autistic symptoms, and its ability to accurately detect changes in symptoms and follow-up is doubtful. On the other hand, the SRS-2 scale is thought to be more reliable in capturing the change in symptom severity over time [23]. However, there is a lack of universally accepted measures and standardization for the assessment tools in ASD trials, which has led to conflicting and inconclusive results.
There was a great variability in the assessment tool used for social interaction and repetitive behavior. There were not enough studies in each subgroup to compare different tools. However, pooled analysis of the different scales using standardized mean differences showed a statistically significant difference. However, when replacing the SRS-2 values in Dai et al. with the ADOS values, the results became non-significant. This could be attributed to the core differences between the two scales. SRS-2 is completed by caregivers and assesses the severity of social impairment related to ASD. It provides a quantitative measure of social behaviors across various contexts, which reflects on the retrospective observations of the child’s social interaction over a certain period. On the other hand, the ADOS scale is a semi-structured observational tool administered by clinicians to obtain direct observation about the child’s social interaction, communication, and other social behaviors related to ASD [24, 25]. This difference could lead to variations in the aspects captured by each scale. Additionally, since the ADOS scale relies on current observations rather than retrospective reporting, it could be more sensitive in detecting immediate changes. However, the retrospective nature of SRS-2 provides valuable insights into the consistent behavioral patterns, which could be more useful in the clinical context.
4.4. Comparison with previous studies
Our meta-analysis addresses several key limitations found in the existing meta-analysis conducted by Wang et al. [7], providing a more accurate and reliable assessment of the treatment effects of bumetanide in children with ASD.
4.4.1. Including recent large RCTs
Our meta-analysis covers three recent RCTs, including two major phase III multicenter studies by Fuentes et al., with a total sample size of over 400 patients, which is approximately equal to the total sample size of Wang’s study. These trials were terminated because they failed to show significant differences between the bumetanide-treated and placebo groups, highlighting the need for a more comprehensive analysis [8]. The inclusion of these trials could potentially affect the overall results.
4.4.2. Methodological flaws in the previous Meta-Analysis
Duplicated samples in the same analysis
One major limitation of Wang et al.‘s meta-analysis is that they combined different subscales measuring social interaction from the same study into a single analysis. This approach has assigned disproportionate weight t certain studies, leading to inflated significance of results that might not hold if analyzed separately (1). Our meta-analysis addresses this limitation and obtains more accurate results by avoiding the inclusion of multiple scales addressing the same domain from a single study and choosing only one scale per investigation to avoid double-counting. Indeed, this approach showed varied significance from the previous meta-analysis. Moreover, it highlights the impact of scale selection on the meta-analysis outcomes due to possible differences in scope, sensitivity, specificity between tests.
Use of post-intervention values
Wang et al. used post-intervention values only, not MD, which do not account for baseline differences and provides less accurate estimation of the treatment effect compared to using the change values which provides more powerful comparison as it eliminates the factor of inter-person variability from the analysis [26]. In contrast, our meta-analysis employed MD and showed no significant difference from the baseline, highlighting the potential overestimation of treatment effects in the previous analysis.
Fixed effect model vs. random effect model
The included studies had heterogeneous populations of different ages, dosages, races, and severity of disease. Moreover, some studies included participants with Asperger syndrome, while others did not. To address this variability, we used a random effects model for more reliable and generalizable results, unlike Wang and his colleagues who used a fixed effects model [27].
4.5. Strengths and limitations
This meta-analysis provides updated evidence regarding the use of bumetanide for ASD, highlighting the individual variations and factors that might affect treatment response. However, this study is not devoid of limitations.
One of the primary limitations is the heterogeneity and the lack of standardized methodology and assessment among the included RCTs. Variations in sample sizes, treatment durations, dosage regimens, and outcome measures, assessed by various scales and tools, complicate the direct comparison across trials. This variability may overestimate or underestimate bumetanide’s efficacy and affect the robustness and generalizability of the results. Additionally, several included studies had relatively small sample sizes, which could lead to imprecise results and potentially biased findings. Moreover, there were some variations in the inclusion criteria among the clinical trials. There was a lack of analysis of a certain subset of patients, such as those with associated ADHD or certain symptom predominance. Therefore, the results may not reflect the general ASD population and do not provide enough evidence regarding the individualized treatment for ASD patients. Although we conducted subgroup analyses for certain scales, we were limited by the sample sizes; therefore, some potentially significant subgroup effects may not have been fully explored. Moreover, several trials included in this meta-analysis had short follow-up durations, limiting the ability to evaluate the long-term effectiveness and safety of bumetanide, which is crucial given the chronic nature of ASD.
The diuretic properties of bumetanide present a challenge to effective blinding. Side effects such as polyuria, reported commonly or exclusively in the treatment arms of several trials, including Dai 2021, Shaker 2024, Zhang 2020, and Lemonnier 2017 might unintentionally reveal treatment allocation to participants or caregivers. Besides, none of the trials formally assessed blinding success, thus increasing the possibility of observer bias, particularly in caregiver-reported measures such as SRS-2. In contrast, outcomes based on structured observation, such as the ADOS, showed no significant effect. This could explain the difference in significance in social interaction and repetitive behavior when using SRS-2 vs. ADOS.
Although some studies used placebo tablets or liquid formulations matched in color, taste, timing, and administration, none employed active placebos (e.g., low-dose diuretics) to mask side effects, possibly due to ethical considerations. Future studies should consider using active placebos and formally evaluating blinding to minimize bias.
4.6. Clinical implications
Although we found a significant difference in favor of bumetanide in CARS and SRS-2, the obtained effect estimate doesn’t provide clinical significance. For instance, the minimal clinically important difference (MCID) in CARS scale and SRS-2 are 4.5 and 10 points, respectively, which is slightly higher than what we reported [19, 28]. Although this MCID was included in our confidence interval, the small sample size and number of trials limit the precision of the results. Moreover, the MCID of SRS-2 was not based on established criteria but rather expert observations [28].


Comments (0)