In the current study, patients received high dose methotrexate from 2022 till 2024 revealed a significant association between the patients with pleural effusions and elevated 48-h MTX levels based on the cutoff value of ≥ 1.28 μmol/L [14]. In agreement with previous studies, patients diagnosed with lymphoma experienced significantly higher 48 h MTX levels [5,6,7] Unlike Donoghue et al., age, sex, and BSA were not found as predictors of high methotrexate level [14].
Reviewing the medical and medication history of the patients showed that both proton pump inhibitors (PPI) and antigout medications have significantly increased MTX level. Evidence indicates that the concurrent use of methotrexate, particularly at high doses, with PPIs and antigout medications may reduce methotrexate clearance. This reduction can result in increased serum levels of methotrexate and/or its metabolite hydroxymethotrexate, potentially causing methotrexate-related toxicities [15, 16].
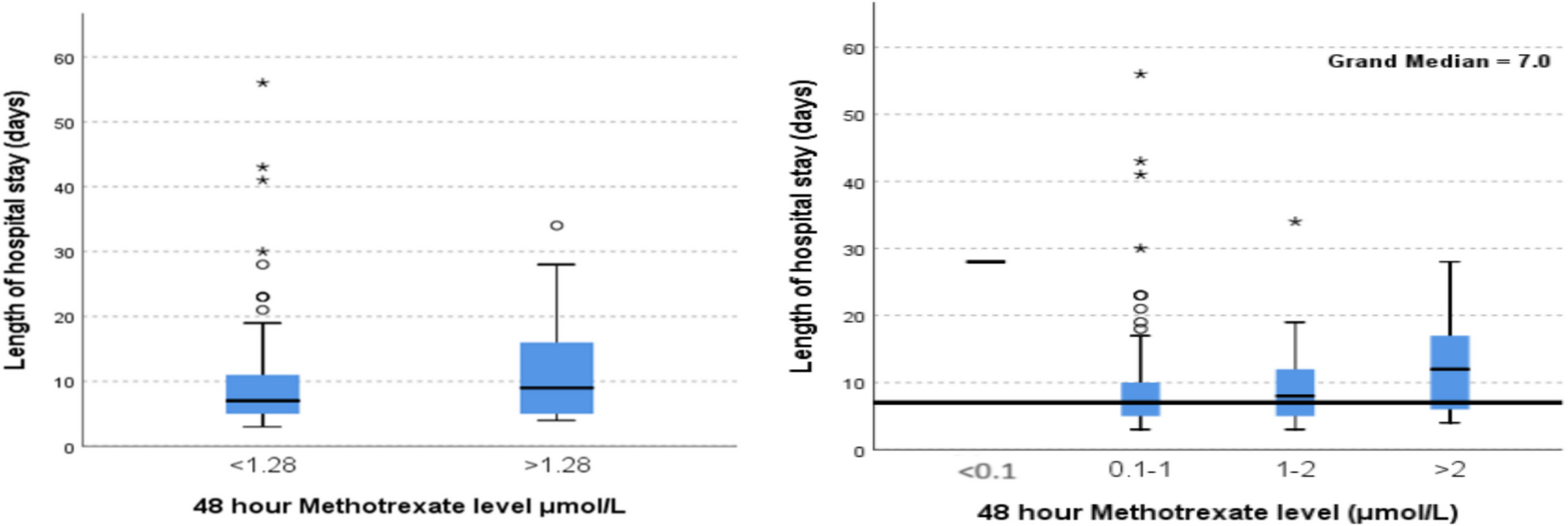
The overall incidence of AKI in this study was 19.5%. Although it is notably higher than the traditionally reported rates of 2% to 12% [5], it is similar to that observed by Donoghue et al., in patients with lymphoma receiving a high dose of methotrexate [14]. In contrast, Wiczer et al. documented a significantly higher nephrotoxicity rate of 39% in their retrospective study of high dose MTX [17]. Additionally, only numerical increase in acute kidney injury and hepatotoxicity was observed with MTX level ≥ 1.28 μmol/L, the lack of significance could be attributed to the small sample size. Furthermore, the median hospital stay length increased with higher MTX levels, are consistent with the findings of Donoghue et al. [13]. Specifically, the median hospital stay was non-significantly longer at 9 days for methotrexate levels ≥ 1.28 compared to 7 days for levels < 1.28. Moreover, the median hospital stay extends from 7 days for a 48-h MTX level of 0.1–1 μmol/L to 8 days for an MTX level of 1–2 μmol/L and further increases to 13.5 days for a MTX level exceeding 2 μmol/L. These findings carry significant short-term implications for hospitalization and ICU admission, potentially delaying subsequent MTX cycles and increasing healthcare costs.
In the current study, both toxicity profiles and hospital stay durations varied according to tumor type. Hepatotoxicity was significantly more common in patients with solid tumors compared to those with hematological malignancies which might be due to the fact that treatment regimens for solid tumors carry a higher risk of liver-related adverse effects. Langman et al., concluded that the cases of methotrexate toxicity might actually be due to nonalcoholic steatohepatitis [18]. Another possible explanation for this finding aligns with the study by Abe K. et al., which identified female sex as a risk factor for hepatotoxicity in patients with osteosarcoma who received MTX [19]. In the currently studied cohort, 38% of osteosarcoma patients were female compared to only 24% in the hematological malignancies group, potentially contributing to the higher rate of hepatotoxicity observed in the solid tumor group. The influence of female sex hormones, along with sex-related differences in methotrexate pharmacokinetics, may partially account for this disparity. In agreement with Wang et al. the co-administration of PPI and NSAIDs have limited non- significant effects on acute hepatotoxicity [20]. On the other hand, other toxicities such as acute kidney injury, disease progression, and 30-day mortality were more frequent in one group or another, but these differences did not reach statistical significance.
Regarding the length of hospital stay and in agreement with previous studies [21, 22], patients with osteosarcoma had a shorter median length of stay compared to those with leukemia and lymphoma. Lymphoma patients showed the greatest variability in hospitalization duration, mostly due to combination of HDMTX with other myelosuppressive chemotherapeutic agents resulting in longer hospital stay.
In this context, the univariate analysis showed significant increase in some antimicrobials with MTX levels ≥ 1.28 μmol/L for the management of nosocomial infections [23, 24]. Notably, the use of carbapenems, vancomycin, and fluoroquinolones showed a significant increase during hospitalization at MTX levels ≥ 1.28 μmol/L (P-value 0.05). Carbapenems are considered the antibiotics of last resort in many regions among β-lactams for human treatment due to their safety and effectiveness in addressing multidrug-resistant (MDR) gram-negative bacterial infections. However, over the past decade, the increasing prevalence of carbapenem resistance has presented a significant challenge for clinicians in managing both community- and healthcare-associated infections [25]. Comprehensive and targeted antimicrobial resistance (AMR) surveillance, with a focus on carbapenem resistance, is urgently needed to create and implement effective national policies aimed at preserving the effectiveness of carbapenems as last-resort antibiotics [25].
Methotrexate is primarily eliminated by the kidneys and in a lesser extent by the liver. Thus, impaired elimination, which can lead to serious toxic effects, may occur due to renal dysfunction caused by inadequate alkaline hydration, consumption of acidic beverages, or drug-drug interactions [26, 27]. The co-administration of some antimicrobials has been shown to delay methotrexate elimination via the kidneys, potentially resulting in severe toxicity. These include the penicillins piperacillin, alone or combined with tazobactam, oxacillin, amoxicillin, mezlocillin, the fluoroquinolone ciprofloxacin, the glycopeptide vancomycin and the streptogramin pristinamycin [26]. Moreover, delayed methotrexate clearance may also be attributed to renal dysfunction secondary to sepsis. In the current study, most antimicrobials were not significantly associated with nephrotoxicity or hepatotoxicity.
The key strengths of this study is its comprehensive evaluation of multiple clinically relevant outcomes associated with HDMTX therapy, including 48-h serum methotrexate levels, nephrotoxicity, hepatotoxicity, antimicrobial use, and hospital stay duration. The inclusion of a relatively diverse patient cohort across different cancer types enhances the generalizability of the findings. Furthermore, the study provides a detailed analysis of the relationship between methotrexate levels and concomitant medication use, particularly antimicrobials, offering valuable insights into potential drug interactions. By incorporating both biochemical data and clinical outcomes, the study delivers a more integrated understanding of HDMTX toxicity in real-world settings, which can support more individualized and safer patient care strategies. However, the limitations of the current study include its retrospective nature and the missed data of some patients.







Comments (0)