
Remember me





The last few decades have witnessed remarkable developments in cancer diagnostics and treatment strategies. Identification of oncogenic drivers and the development of targeted therapeutic agents have shifted the paradigm of cancer care. This phenomenon of the molecular profiling of tumor cells to identify the oncogenic alterations is widely known as precision oncology [1]. Non-small cell lung cancer (NSCLC) has been exemplified as the prototype disease for precision oncology in solid tumors. This was the result of the identification of epidermal growth factor receptor (EGFR) mutations which led to the inclusion of EGFR tyrosine kinase inhibitors (TKIs) into the treatment regimen of patients with EGFR mutant NSCLC [2].
The NSCLC is a heterogeneous malignancy involving a large number of oncogenic driver alterations. NSCLC accounts for nearly 85% of lung cancer cases and is further divided into adenocarcinoma (NSCLC-AC), squamous cell carcinoma (NSCLC-SCC), and large cell carcinoma [3]. More than half of the cases of NSCLC are diagnosed at an advanced stage and suffer from poor prognostic outcomes with a 5-year survival rate of only 2–20% [4]. Currently, targeted therapeutic agents are considered the standard of care for most NSCLC patients with molecular alterations [5]. For patients without any actionable oncogenic mutations, immunotherapy with programmed cell death ligand-1 (PD-1/PD-L1) and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) is utilized as the treatment of choice [6]. Nevertheless, the majority of patients treated with immunotherapy or targeted therapy agents develop resistance or relapse following a few years of treatment and require alternative therapeutic strategies, necessitating the need for novel treatment approaches [7].
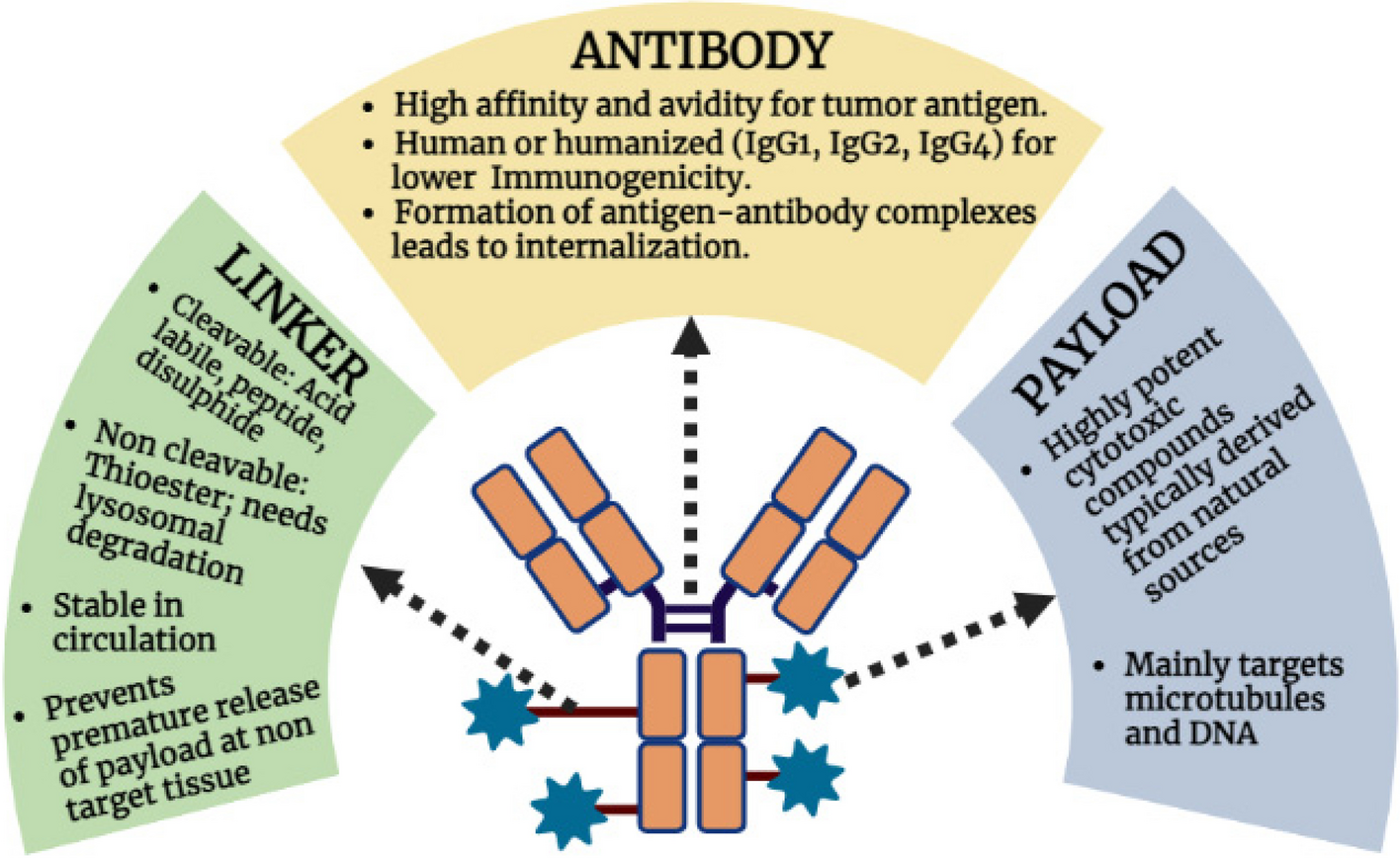
Antibody–drug conjugates (ADCs) are a unique therapeutic ensemble combining the target selectivity of monoclonal antibodies (mAb) with the cytotoxic effects of chemotherapeutic agents [8]. In order to assemble a safe and efficacious ADC, a meticulous selection of antibodies, payload, and the connecting linker moiety is essential [9]. The structural bifurcation and properties of each component of an ADC have been provided in Fig. 1. The mechanism of action of ADCs is multifaceted, involving several steps (Fig. 2). Firstly, the mAb binds with the target antigen exclusively present in the cancer cell, in order to reduce the off-target toxicities. This ADC-antigen complex is then internalized into the cell followed by lysosomal fusion and cytotoxic drug release into the cell. The cytotoxic payload of an ADC comprises microtubule disrupting agents, topoisomerase inhibitors, or DNA cleavage agents, which are responsible for the resultant cytotoxicity [10]. The structural layout of various ADCs currently under investigation in NSCLC is summarized in Table 1. In addition to the cytotoxic effects exerted on the antigen-positive tumor cells, the metabolites of cytotoxic agents might permeate through the membrane and kill adjacent tumor cells by their bystander-killing effects. This anomaly can offer a significant advantage when a target heterogenicity is observed within the tumor microenvironment (TME) and not all tumor cells sufficiently express the target antigen [11]. ADCs have successfully paved their way into the therapeutic regimen of several malignancies, including breast cancer and gastric cancers following their Food and drug administration (FDA) approvals. Numerous ADCs are currently under development in lung cancer patients with promising results from phase I–II clinical trials [12].
Fig. 1
Structural bifurcation of ADCs along with their properties. Immunoglobulin (Ig), Deoxyribonucleic acid (DNA)
Fig. 2
Summary of different oncogenic biomarkers and effective antibody–drug conjugates in patients suffering from non-small cell lung cancer
Table 1 Structural layout of ADCs currently under development in NSCLCThis review presents an elaborate discussion regarding the utilization of ADCs in NSCLC. Numerous biomarkers responsible for the development of NSCLC along with their oncogenic mechanisms have been discussed thoroughly. This review focuses on the respective ADCs working on those specific biomarkers in NSCLC along with the evidence retrieved from the clinical trials.
Promising ADC targets for the treatment of NSCLCc-METc-Mesenchymal-epithelial transition factor-1 (c-MET) is a transmembrane tyrosine kinase receptor and an oncogenesis driver explored as a potential target by anti-cancer moieties for delivering anti-tumor activity [13, 14]. Alternatively termed as Hepatocyte growth factor (HGF) receptor, it encodes a protein tyrosine kinase which holds responsibility for regulating important cellular processes namely cell differentiation, cell proliferation, cell division, movement, and apoptosis. HGF expression is carried out by stromal and mesenchymal cells and is a paracrine signaling molecule which solely acts as a ligand for c-MET [15]. In tumor cells, the activation of MET occurs in multiple ways including receptor and ligand overexpression, gene amplification, gene mutation, and rearrangements in chromosomes. Two primary forms of MET expression showing a potential association with the progression of NSCLC are (1) MET exon 14 skipping alteration and (2) MET gene copy number gain (CNG) [16]. Moreover, MET gene amplification is an identified culprit defined to induce resistance toward EGFR-targeted therapies [17]. MET alterations have the most tendency to be involved in NSCLC-AC courses while they are also prevalent in NSCLC-SCC. Nearly 5% of NSCLC patients show MET exon 14 skipping. On the contrary, a very low percentage of patients have MET gene amplification. MET exon 14 skipping and MET amplification both can be diagnosed through comprehensive next-generation sequencing (NGS) and fluorescence in-situ hybridization (FISH) [18]. The silencing of MET through small interference RNA or short hairpin RNA or inactivation of the biomarker through micro-RNAs has been stated as prominent in vitro for cell viability, downstream signaling, cell motility, migration, and invasion [19]. Extensive efforts have been made on MET inhibitors considering pre-clinical models to further lead a direction for clinical studies investigating these agents. Drawing evidence from a study exploring c-MET receptor expression in NSCLC cell lines, the methodology involved evaluation of c-MET receptor through the employment of western blot analysis [20]. 11 established cell lines and 104 surgically resected tissues were subjected to western blot where the cell line distribution consisted of 8 adenocarcinomas, 2 squamous cell carcinomas and a large cell carcinoma [21]. The NSCLC tissues used for the study were obtained from 104 patients, were frozen, and kept at − 80 °C. For western blotting, each NSCLC cell line was formerly harvested at the exponential growth phase. Immediately the cell pellet was homogenized in 1 ml of 10 mM Tris-HCl buffer [22]. The homogenate was later centrifuged at 10,000 rpm for 15 min at 4 °C and the clear supernatant, thus obtained, was used for western blotting. All cell lines affirmed a strong presence of c-MET proteinaceous bands of 145 kDa and 170 kDa. The clarity of results was found slightly lacking as two cell lines used in this study originated from negative c-MET expression also suggested its presence which may be justified as a consequence of cell line influence during cultivation. The conclusion of this clinicopathological study also revealed that NSCLC positive for c-MET expression may present worse outcomes as compared to NSCLC without c-MET involvement [23].
A conventional c-MET inhibitor such as small molecule TKIs delivers potential anti-tumor efficacy in several tumor cell lines expressing higher HGF concentrations over 50 ng/mL. The tumor cell lines expressing lower HGF levels in human serum ranging between 0.4 to 0.8 ng/mL remain undetected by c-MET inhibitors as the sensitivity of conventional therapies diminishes at such non-physiological concentrations [24]. On the other hand, these TKIs show limited implications on therapeutic regimens due to the emergence of acquired resistance.
For the detection of such lowly expressed c-MET biomarkers, the concept of ADCs presents an affirmative potential. A summary of different oncogenic biomarkers and ADCs targeting them in NSCLC patients has been provided in Fig. 2. The current drug ecosystem has developed three such ADCs targeting c-MET mutation and amplification phenomena.
Telisotuzumab vedotin (Teliso-V), formerly named ABBV-399, holds FDA approval for the treatment of advanced/metastatic stage of EGFR wild type, nonsquamous NSCLC positive for c-MET mutation [25, 26]. Following the encouraging data from the LUMINOSITY (NCT03539536) phase 2 trial, Telisotuzumab vedotin received breakthrough therapy designation (BTD) from the FDA for previously treated NSCLC with c-MET overexpression. This trial included 136 patients with advanced NSCLC who were further divided into cohorts based on their histopathological examinations (non-squamous [NSQ] or squamous [SQ], EGFR mutation status [wild-type or mutant]). The NSQ cohort further subdivided patients based on whether the c-MET expression was high or intermediate. The study is being carried out in two stages. Stage 1 was focused on identifying that which c-MET overexpressing NSCLC populations were most suitable for Telisotuzumab vedotin. The results demonstrated an overall response rate (ORR) of 36.5% in the NSQ EGFR-WT cohort (52.2% in the c-MET high and 24.1% in the c-MET intermediate population). The NSQ EGFR mutant and SQ cohort showed only modest improvements. Serious adverse events were seen in two patients from the SQ cohort in the form of sudden death and pneumonitis [27]. From this trial data, it can be concluded that the histopathological examinations play a crucial role in determining the response to the therapy as the NSQ cohort with WT-EGFR had the best response. Moreover, the c-MET intermediate population also showed improvements from the therapy, which demonstrates the potential of ADCs in targeting not only the high-expressing cells but also the moderate expression present in the target cells. Another phase 2 trial Lung-MAP S1400K evaluated the outcome of administering Tisotuzumab vedotin in patients with c-MET positive previously treated squamous cell lung carcinoma. Patients were divided into 2 cohorts based on their previous exposure to immune checkpoint inhibitors (ICIs). The patients received 2.7 mg/kg dose of Tisotuzumab vedotin every 3 weeks until the occurrence of unacceptable toxicities or disease progression. The results were disappointing as the median overall survival (OS) and progression-free survival (PFS) were 5.6 months and 2.4 months with only two responses reported in the immunotherapy naïve cohort. Additionally, two patients developed pneumonitis resulting in death. The trial was discontinued owing to the lack of efficacy which did not justify the further evaluation [28]. Thus, from the above two discussed studies it can be inferred that Tisotuzumab vedotin has failed to produce significant responses in the patients with squamous cell carcinoma. However, these results have not blocked further studies for Tisotuzumab vedotin in c-MET positive NSCLC patients as currently, many trials are under investigation which is expected to derive substantial outcomes soon. Evidence from the completed clinical trials evaluating the application of ADCs in NSCLC is summarized in Table 2.
Table 2 Clinical data on the use of ADCs in NSCLCREGN5093-M114 is another ADC efficient for targeting the acquired MET-amplification driving the NSCLC tumor progression [29]. A phase I/II, open-label study (NCT04982224) is currently under investigation for evaluating the role of REGN5093-M114 in advanced NSCLC patients showcasing MET-overexpression [29]. Positive outcomes from this study can embark upon a detailed investigation of this molecule in MET-overexpressing NSCLC patients.
MYTX-011 is one additional ADC working by diminishing MET amplification contributing to carcinogenesis. A phase 1 study (NCT05652868) is currently under investigation to assess the safety, tolerability, and preliminary effectiveness of MYTX-011 in patients with advanced, recurrent, or metastatic NSCLC [30]. Currently, ongoing clinical trials of various ADCs for the use in NSCLC are presented in Table 3.
Table 3 Currently ongoing trials evaluating ADCs in NSCLCTROP-2Human trophoblast cell-surface antigen 2 (TROP-2) is a promising molecular biomarker owing to its high expression in numerous epithelial carcinomas including NSCLC [31]. Encoded by the tumor-associated calcium signal transductor (Tacstd2) gene, TROP-2 is a transmembrane glycoprotein and an intracellular calcium signal transducer with downstream signaling supporting cell survival, promoting proliferation and migration along with invasion in tumor cells [32]. Overexpression of TROP-2 is more commonly observed in NSCLC-SCC than in lung adenocarcinoma which is independent of sex, histologic grade, and pathologic stage [33]. The presence of this overexpression is associated with poor prognosis and lung cancer-specific mortality. Formerly mentioned substantiations have been derived from a study investigating TROP2 as a potential prognostic marker and therapeutic target. The in-vitro study included human bronchial epithelial cells and NSCLC cell lines. The NSCLC cell lines were cultured in RPMI 1640 (Gibco, Invitrogen Life Technologies, Carlsbad, CA, USA). The tissue samples and adjacent normal tissue samples were obtained post-retrieval of informed consent from 20 patients. These samples were further snap-frozen in liquid nitrogen followed by immunohistochemical staining using the standard streptavidin-biotin-peroxidase complex method. The construction of TROP-2 silenced and overexpressing cell lines was practiced after which the real-time quantitative reverse transcription PCR, western blot, wound healing assay, cell proliferation assay, transwell migration assay, and flow cytometry assay were performed. The results reported TROP-2 overexpression which correlated significantly with clinical stage, differentiation, lymph node metastasis, and distant metastasis [34]. The study affirmed TROP-2 as an oncogene in lung adenocarcinoma.
At present, there are three ADC molecules (Datopotamab deruxtecan, Sacituzumab govitecan, and SKB264) under investigation, which can identify and target TROP-2.
Datopotamab deruxtecan, otherwise known as Dato-DxD and DS-1062a, was evaluated in the TROPION-PanTumor01 (NCT03401385) trial. The results of the dose escalation/expansion phase in patients with advanced NSCLC exhibited a disease control rate (DCR) of 87%, ORR of 21%, and median PFS of 8.2 months along with a manageable safety profile. However, interstitial lung disease (ILD) was observed in 8 patients. The 6 mg/kg dose of Dato-DXd as monotherapy is currently under phase-III trial [35].
TROPION-Lung02 (NCT04526691) trial is currently evaluating the combination of Dato-DXd and Pembrolizumab with or without chemotherapy in treatment naïve or previously treated subjects with metastatic/advanced NSCLC [36]. Evaluating this combination in the treatment of naïve patients is crucial and can significantly improve the treatment strategies for patients with advanced NSCLC in the future.
Another phase-III trial called TROPION-Lung08 (NCT05555732) is assessing the superiority of Dato-DXd combined with Pembrolizumab compared to Pembrolizumab alone in treatment naïve patients with metastatic/advanced NSCLC without actionable genomic alterations. Nearly 740 participants will be enrolled whose tumor expresses high PD-L1 expression (> 50%). The primary endpoints of the study are PFS and OS [37].
The majority of discussed trials above focus on the treatment of naïve patients with advanced NSCLC. Affirmative outcomes from these studies have the potential to alter the treatment landscape of patients suffering from advanced NSCLC, by incorporating the ADCs and immunotherapeutic agents in the earlier lines of therapy where the odds of achieving improved prognostic outcomes are significantly higher.
Sacituzumab govitecan-hziy (SG) has proven its efficacy and superiority over other therapeutic modalities in various cancers including metastatic triple-negative breast cancer (mTNBC). Following the encouraging data from numerous clinical studies, SG received accelerated approval from the FDA for treatment in mTNBC. At present, several studies are evaluating the safety and efficacy of the same in patients with NSCLC. The IMMU-132-01 trial assessed the safety and antitumor efficacy of SG in patients with advanced epithelial cancers which included the NSCLC cohort. The study enrolled patients with metastatic NSCLC who were heavily pre-treated with other therapeutic modalities including ICIs. The patients were treated with 8 mg/kg or 10 mg/kg dose of SG on days 1st and 8th of a 21-day cycle. The median response duration from the treatment was 6 months along with an ORR of 16.7% and a clinical benefit rate (CBR) of 24.1%. Partial response (PR) was observed in 9 patients and complete response (CR) was not observed at all. Additionally, median PFS and median OS were 4.4 months and 7.3 months, respectively. The most commonly observed adverse events (AEs) were neutropenia and diarrhea, which were generally tolerable with dose reductions. The patients who progress after two or more lines of therapy in the metastatic setting generally face dismal prognostic outcomes and have very few treatment options apart from palliative care. The encouraging results from this trial hint toward the addition of SG in the treatment regimen for the heavily pre-treated patients with advanced disease. One significant limitation of this trial was the absence of immunohistochemistry (IHC) analysis to assess the TROP-2 positivity [38]. Assessing the impact of TROP-2 expression on the antitumor activity of SG can aid in selecting the patient population that can benefit the most from the treatment. Thus, future clinical studies evaluating SG should aim to focus on correlating the TROP-2 expression with the antitumor responses of the drug.
CEACAM-5Carcinoembryogenic antigen-related cell adhesion molecule-5 (CEACAM-5) belongs to the CEACAM group with highly glycosylated proteins possessing a typical N-terminal variable Ig domain and is located on the cell surface [39]. CEACAM-5 is found to have an inhibitory action on p38 activity which regulates multiple complex biological processes such as cell proliferation, cell differentiation, death, migration, and invasion [40]. CEACAM-5 has been noted as a tumor biomarker and recurrence detector in cancer patients, especially those suffering from colorectal carcinoma [41]. Pre-clinical studies had been designed to unveil CEACAM-5 utility in NSCLC. The in vitro and in vivo study performed focusing on the formerly mentioned aim investigated the role of CEACAM-5 in NSCLC progression [42]. Tumor samples, post-isolation were fixed with paraformaldehyde, embedded in paraffin, and cut into 5 µm sections. The following procedures included deparaffinization, rehydration, and incubation for 10 min. Blocking of samples was undertaken using 1% normal goat serum which later was followed by treatment with CEACAM-5 antibody. After immunohistochemistry, several other tests such as real-time quantitative reverse transcription PCR, immunoblotting, cell viability and colony formation assay, wound healing assay, and animal experiments on nude mice were also performed. The study presented findings in the form of an over-expression of CEACAM-5 in human NSCLC tissues and cells. The expression was also found to be correlated with the clinicopathological status of NSCLC patients. The expression of CEACAM-5 and its role in driving the NSCLC oncogenesis was also verified and the in vitro and in vivo study results demonstrated the involvement of the p38-Smad2/3 signaling pathway [39]. Hence, this biomarker was deduced to be a potential therapeutic target for the treatment of NSCLC.
The first-in-human study (NCT02187848) of a novel ADC Tusamitamab ravtansine (SAR408701) demonstrated a favorable safety profile along with ORR of 22.7% in patients with heavily pretreated solid tumors with more than 50% tumor cells expressing CEACAM5 [43]. Building on this premise, this ADC was further evaluated in 92 patients with non-squamous NSCLC having moderate to high CEACAM5 expression. The results demonstrated PR in nearly half of the treated patients even after more than 1 year of treatment [44]. These observations hint toward a durable response and long-term benefit even in previously relapsed patients, which is highly uncommon in patients with advanced malignancies.
EGFREGFR, is a tyrosine kinase receptor belonging to the ERBB family [45]. When an extracellular ligand binds to EGFR, it triggers the receptor to undergo homo- or heterodimerization, leading to phosphorylation of tyrosine kinase sites within the cytoplasm. This, in turn, initiates various intracellular pathways, including the PI3K/AKT/mTOR and RAS/RAF/MAPK which control cell proliferation and metastasis and prevent apoptosis [46]. The majority of the EGFR mutations in NSCLC have been identified in exons 18–21 of the tyrosine kinase domain of the receptor, which encode for a portion of the EGFR kinase domain. EGFR 19 deletion or an EGFR L858R point mutation is frequently observed in NSCLC cases [47]. The less prevalent EGFR mutations include G718X, S768I and L861Q. A special type of EGFR mutation—in-frame insertion in exon 20 (T790M)—occurs in 3–7% of NSCLC cases. EGFR mutations are commonly found in females, never smokers or are light smokers, those of Asiatic origin, and those with NSCLC-AC (10–35%) that have advanced to a locally advanced or metastatic stage (Stage III–IV) [48]. The analysis of EGFR mutations is primarily performed using direct sequencing of DNA and real-time polymerase chain reaction (RT-PCR)-based assays. Both methods demonstrate high performance in detecting these mutations in tissues that have been fixed in formalin and embedded in paraffin. Another method for detecting EGFR mutations is fragment length analysis, which is capable of identifying insertions or deletions but cannot detect point mutations in the EGFR gene [49]. The standard approach for treating advanced or metastatic disease in patients with EGFR-mutant tumors is the use of first- or second-generation EGFR TKIs as initial therapy. The first-generation TKIs, such as gefitinib and erlotinib, are reversible inhibitors that demonstrate strong inhibitory activity against both the wild-type EGFR and sensitive mutant EGFR. In contrast, the second-generation TKIs, including afatinib and dacomitinib, are irreversible inhibitors. Studies have shown that these TKIs lead to a significantly higher ORR and longer PFS compared to first-generation TKIs. However, there is no significant change in OS with the use of second-generation TKIs [50]. The use of TKIs is limited due to dose-limiting toxicity and the development of resistance in patients [51]. In the treatment of NSCLC patients who are T790M-positive and resistant to earlier-generation TKIs, the third-generation EGFR-TKI osimertinib has become the standard approach [52]. Osimertinib is associated with relatively milder gastrointestinal and skin toxicity compared to previous TKIs [53]. EGFR-mutant tumors, on the other hand, do not respond well to checkpoint inhibitors targeting PD-1 or PD-L1. Therefore, the use of immunotherapy alone is not recommended [54]. Due to the toxicity and development of resistance associated with conventional therapies, the use of ADCs is gaining interest.
MRG003 is currently being investigated for the treatment of EGFR-positive advanced NSCLC. A phase II study is underway to evaluate the effectiveness of MRG003 in patients with EGFR-positive advanced NSCLC. This study aims to gather valuable information about the efficacy, safety, and overall therapeutic potential of MRG003 in treating advanced NSCLC patients with EGFR-positive tumors [55].
HER-2The human epidermal growth factor-2 (HER-2) gene, also known as ErbB2, is a proto-oncogene belonging to the ERBB receptor tyrosine kinase family. HER2 alterations can occur in three forms: gene amplification, overexpression, and point mutations [56]. These mutations are more commonly observed in lung adenocarcinomas, particularly in females, Asians, and individuals who are either never smokers or light smokers [57]. The highest prevalence of these mutations is observed in stage III-IV NSCLC patients. Exon 20-point mutations, namely L755S and G776C, are the most frequently observed HER2 mutations, while other less common mutations include G660D, R678Q, E693K, and Q709L. HER2 mutations can be detected through RT-PCR or gene sequencing methods like NGS. HER2 amplification is identified using FISH analysis, enzyme-linked immunosorbent assay (ELISA), or NGS, while HER2 overexpression is detected through IHC [58]. Treatment options for HER2-mutant tumors include HER2-TKIs, anti-HER2 antibodies, and ADCs. HER2-TKIs are associated with safety concerns and tolerability issues [56]. ADCs are gaining attention due to their limited toxicity and high tumor selectivity [59].
Trastuzumab Emtansin (T-DM1) is an ADC approved by the FDA for patients with HER-2-positive breast cancer. However, the data for the same in the NSCLC have not been conclusive yet.
A phase-II basket trial (NCT02675829) enrolled 18 patients with adenocarcinoma subtype whose tumors expressed HER2 mutations. These subjects were treated with 3.6 mg/kg T-DM1 every 3 weeks. The results showcased a median PFS of 5 months and a partial response rate of 44%. Commonly observed toxicities were elevation in hepatic transaminase enzymes, thrombocytopenia, and infusion-related reactions. After nearly a decade of unfavorable results from studies targeting HER2 in lung cancer, these results offered several essential insights and embarked upon further trials of ADCs targeting HER2 in lung cancers [60].
A phase II clinical trial (NCT02289833) by Peters et al. evaluated T-DM1 in patients with pretreated advanced NSCLC showcasing HER-2 overexpression. The 49 enrolled patients in this study were divided into two cohorts based on IHC2+ and IHC3+ expression. The results demonstrated favorable clinical outcomes in the IHC3+ cohort compared to the IHC2+ cohort. In the IHC3+ cohort, reported ORR and CBR were 20% and 30%, respectively. However, there was no significant difference between the mPFS and mOS observed in both cohorts, which indicates that IHC grade is not a definitive predictor of efficacy.
Following encouraging outcomes from these trials, T-DM1 was given a category 2A recommendation from the National Comprehensive Cancer Network (NCCN) for the treatment of patients with advanced NSCLC harboring HER2 mutations [61].
Trastuzumab deruxtecan (T-DXd) is a topoisomerase-I inhibitor that is a widely utilized HER2 targeting agent in various malignancies as it is approved by the FDA for use in metastatic or advanced HER2-positive breast cancer and in advanced HER2-positive gastric cancer which is trastuzumab refractory.
A phase-II clinical trial (NCT03505710) by Li et al. evaluated the clinical outcomes of T-DXd in 91 patients with refractory HER2 mutant NSCLC. The results revealed an ORR of 55%, mDoR of 9.3 months, mOS of 17.8 months, and mPFS of 8.2 months. The safety analysis showed the occurrence of grade > 3 AEs in 46% of patients and the occurrence of ILD in 26% of patients. Moreover, ILD resulted in mortality in 2 patients. An intriguing observation from this study was that the efficacy of T-DM1 was observed in even those patients who had HER2 mutation but the IHC grade was 0 (lack of detection of HER2 expression). These observations might be the result of activating HER2 mutations leading to the enhancement of the intracellular uptake of ADC-HER2 receptor complex and receptor internalization [62]. However, further studies are mandatory to procure insights regarding the HER2 expression and clinical efficacy of ADCs.
The DESTINY-Lung02 trial (NCT04644237) compared the safety and efficacy profile of 5.4 mg/kg and 6.4 mg/kg of T-DXd in patients with pretreated NSCLC with HER2 mutation. The interim analysis of the data was presented at the 2022 European Society of Medical Oncology (ESMO) meetings. The results demonstrated ORR of 53.8% and 42.9% in the 5.4 mg/kg and 6.4 mg/kg cohort, respectively. Analysis of the safety data showed that the treatment-emergent adverse events (TEAEs) were higher in the 6.4 mg/kg cohort, with 14% of the patients in this cohort developing ILD. Thus, these results exhibited encouraging clinical activity of T-DXd in patients with NSCLC alongside a promising safety profile in the 5.4 mg/kg cohort. The encouraging results from this study led to the FDA approval of T-DXd at 5.4 mg/kg dose in patients with pretreated HER2-mutant NSCLC [63].
As reported from the previously discussed studies, the occurrence of ILD remains a huge challenge while treating patients with T-DXd. Thus, it is crucial to identify the potential risk factors for developing the ILD as it has proven to be fatal in many patients. Additionally, it was reported that the incidence of ILD was higher in patients with lung cancer when compared to breast cancer or gastric cancer cases. This can be attributed to the preexisting damage to the lung tissue owing to smoking, radiation, or surgery le
Comments (0)