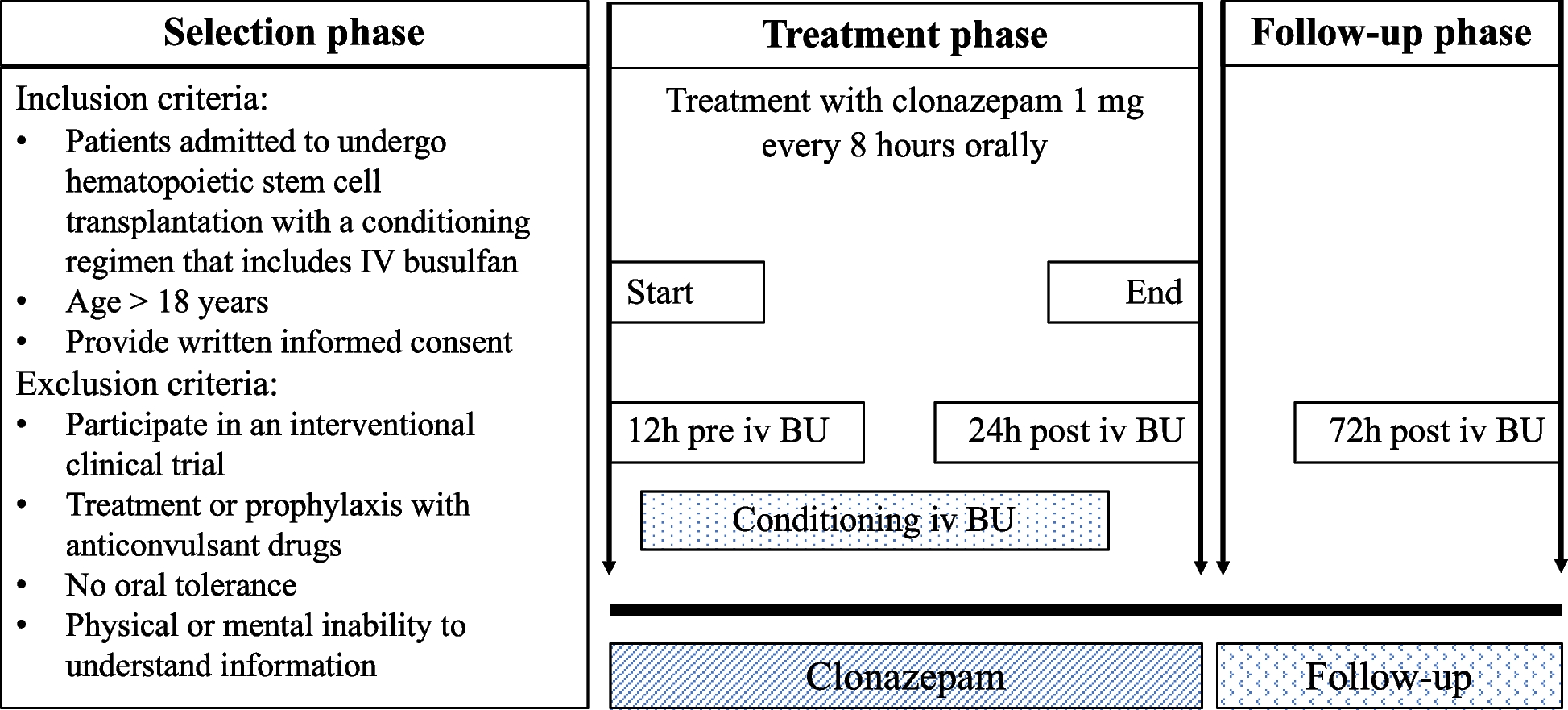
To the authors’ knowledge, we present the results of the largest prospective series to date, with 64 patients, for the evaluation of seizure prophylaxis other than phenytoin in patients treated with high-dose busulfan. The effectiveness was 100%, similar to the previous study with the same drug administered by IV route [16], and higher than historical data with phenytoin, which establish seizure frequency at between 0 and 5.5% [3]. The clonazepam treatment period ranged from 2.5 to 5.5 days, with the specific duration dependent on the number of days of busulfan administration. The absence of seizures over the course of treatment suggests that tachyphylaxis did not occur.
Comparison of results with other studies is difficult since prophylaxis doses, times, and intervals, as well as busulfan doses and route of administration, vary greatly.
In a retrospective, multicentric series that includes 954 HSCT procedures in pediatric patients, 66% of which were treated with oral busulfan and 34% of which were treated with IV busulfan, Caselli et al. [20] describe a seizure incidence of 1.3%, with 0.52% attributed by the authors to the drug. In this study, all the patients received prophylaxis with a high variety of drugs and dosing regimens (carbamazepine, clonazepam, valproate, phenobarbital, lorazepam, etc.).
Compared to other studies with benzodiazepines, it is worth mentioning the review by Eberly [3] which includes several studies with different benzodiazepines and different doses and dosing regimens; the study reviews small series (8–46 patients), mainly pediatric, with seizure results varying between 0 and 4.5% of patients (note that in the two studies reporting seizures, one case was that of a child who had not received the intended benzodiazepine and the other of a patient who had a history of seizures and was receiving concomitant carbamazepine). Carreras et al. [6] used clonazepam IV, administered in continuous perfusion, in 24 adult patients, with the aim of studying the possible influence of this prophylaxis on the pharmacokinetics of IV busulfan. No cases of seizures occurred in their study. On the other hand, Tsujimoto et al. [21] retrospectively compared clonazepam (n = 13) with levetiracetam (n = 30) in children. In their study, they describe no cases of seizures in the clonazepam-treated series, while there were two cases in the levetiracetam group (6.7%). The differences are not statistically significant, given the small sample size.
Other studies using levetiracetam prophylaxis do not describe seizures: Akiyama et al. [13] did not observe any cases in 34 adult patients treated with levetiracetam, while 1 patient out of 70 treated with phenytoin developed seizures in their retrospective series. Similarly, Nakashima et al. [12] did not describe any cases of seizures in a series of 46 adult patients treated with levetiracetam, neither did Chaguaceda et al. [14] in 36 adult patients receiving 1000 mg every 12-h doses of levetiracetam nor did Floeter et al. [22] in 9 pediatric patients, or Soni et al. [23] in a cohort of 28 children and young adults, using IV levetiracetam. These series, although all of them retrospective, reported reasonable outcomes.
Although the use of prophylaxis in this context is widely established, some authors question its use [24], arguing that there are also data on the occurrence of seizures despite the use of prophylaxis [5, 20] and based on their experience of minimal incidence without prophylaxis (0.01%, 1 case out of 96), in a retrospective series, with busulfan administered orally. Ruiz-Arguelles et al. [25] also question the need for anti-seizure prophylaxis in all conditioning settings; in their experience with 344 patients conditioned with a reduced-intensity regimen (oral busulfan 8 mg/kg over 2 days), they observed no cases of seizures.
Tolerance of the scheduled oral clonazepam regimen was very good, so the oral route was maintained in 100% of the patients, and it was only necessary to reduce the dose in 3.1% of patients, due to the clinical criterion of excessive drowsiness, albeit classified as moderate.
Most adverse events described during the follow-up period were frequently associated with other conditioning and supportive therapy components that are well-known for their toxicity profile: nausea and vomiting associated with chemotherapy, hyperglycemia associated with the use of corticosteroids, transaminitis associated with busulfan or fluconazole, or reactions associated with ATG infusion.
All benzodiazepines are associated with sedation and poor coordination. None of these is commonly associated with hematological, dermatological, or hepatic toxicity [3]. The adverse events most likely to be associated with to clonazepam were somnolence (40.6%), dizziness (18.8%), and confusion (10.9%), mostly mild. It is worth noting the involvement in these events of other CNS depressant drugs prescribed simultaneously, albeit on an ad hoc basis, particularly dexchlorpheniramine and chlorpromazine. The use of these combinations should be limited, and patients should be closely monitored if their administration is essential. One caution that should also be considered with clonazepam is the potential for falls and stumbles due to somnolence, vertigo, and decreased muscle tone, although these were not reported in this study.
Other studies do not present a comprehensive description of adverse events during the period of prophylaxis administration, but focus on how prophylaxis affects typical conditioning toxicity (HSOS, oral mucositis, pulmonary toxicity, etc.) [13, 23], or describe the toxicities to be expected with the drug used in prophylaxis [12, 14, 21], in particular neurological events. Tsujimoto et al. [21] describe more frequent somnolence (46%) and dizziness (54%), together with 62% irritability, in their pediatric population treated with clonazepam, while they observed less, but not statistically significant, somnolence with levetiracetam (20%), with no cases of irritability or dizziness in this group. Nakashima et al. [12] describe 19.5% somnolence with levetiracetam, with no indication of the grade; Chaguaceda et al. [14] indicate that the most frequent adverse effects are somnolence, without specifying a percentage, and irritability (11.1%, without mentioning the grade), while Soni et al. [23] only report that they did not observe excessive somnolence or behavioral changes. Other studies have described percentages of somnolence around 50% with lorazepam [7], 9% with phenytoin, or 12.5% with valproic acid [12].
This study is mainly limited by its single-center and non-comparative nature, as well as by a range of conditioning of different intensities, which could be associated with various levels of seizure risk [25]. Plasma busulfan levels were not monitored, as in most published studies [12,13,14, 16, 24, 25], although monitoring could reduce the risk of this and other toxicities [2, 26]. Another suggested option is the inclusion of pharmacogenetic studies to guide dosing, with the aim of increasing the effectiveness and reducing the toxicity of high-dose busulfan. However, this practice has not yet been standardized [27].







Comments (0)