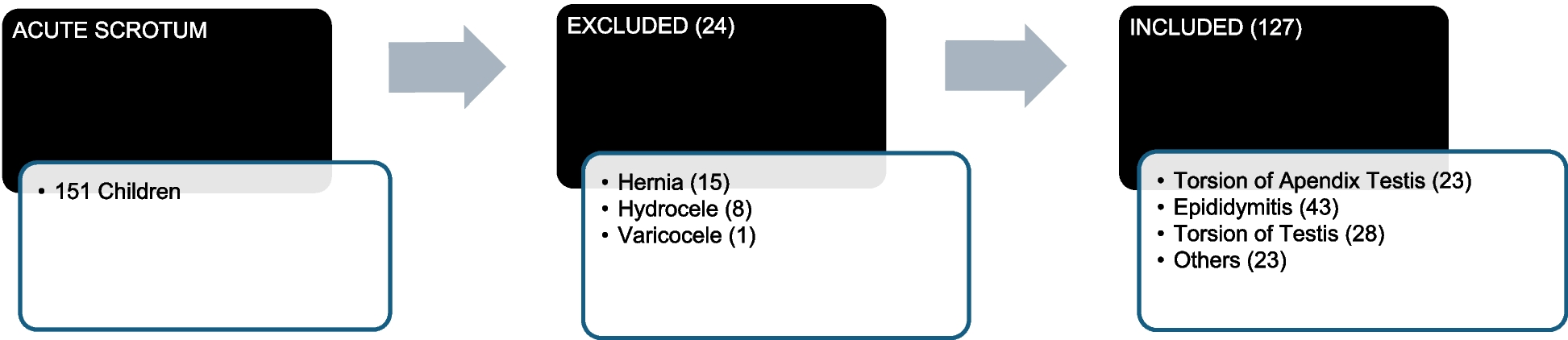
Children with IEI are a heterogeneous group of genetic disorders highly susceptible to infections due to their impaired immune systems. However, the prevalence of non-infectious warning symptoms is not identified among the pediatric population. Our study evaluated 100 children suspected of IEI, of whom 22% were confirmed. In our study, hepatosplenomegaly was the most prevalent non-infectious warning sign, with a strong correlation with ALPS and CVID patients.
The male predominance (72.7%) in our study is consistent with the X-linked mode of inheritance among many IEIs, such as Wiskott-Aldrich syndrome (WAS) and X-linked agammaglobulinemia (XLA) [9]. This predominance aligns with previous studies, such as Alzyoud et al. [6], who reported a male-to-female ratio of 1.3:1 in IEI patients, and Dąbrowska et al. [10], who found that 61.6% of IEI cases were males. Nonetheless, the IEI suspicion index should remain high among females and older age groups, and should not be overlooked.
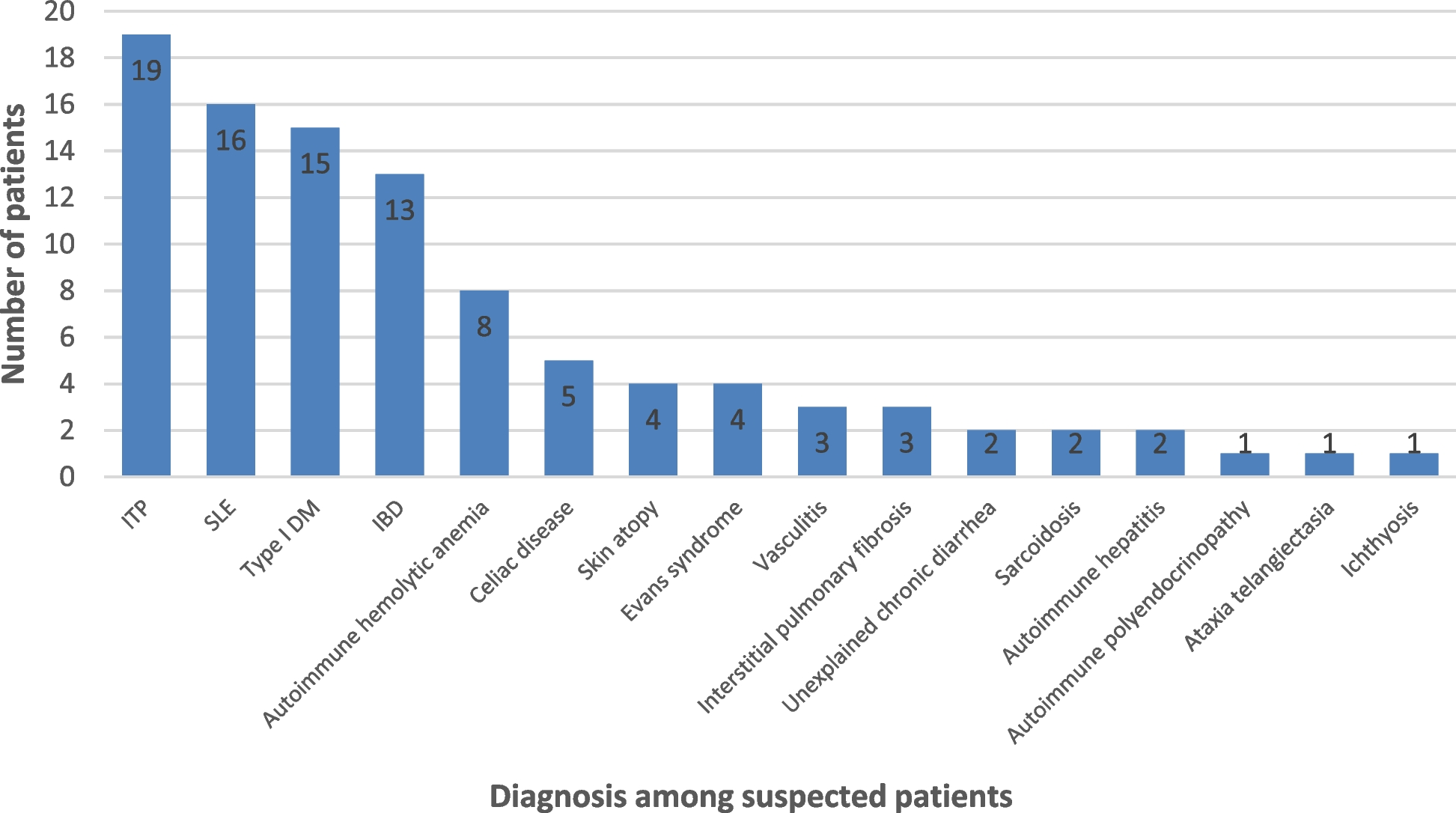
Children with autoimmune and immune-mediated disorders were diverse in our population, where ITP, SLE, and type 1 diabetes were the most commonly identified disorders. Among those disorders, 22 cases of IEI were identified with a wide diagnostic heterogeneity. ALPS was the most commonly identified IEI in our population, followed by adenosine deaminase 2 deficiency, DOCK8 deficiency, and CVID. This highlights the importance of early recognition of immunological disorders and the characteristic features of suspected IEI disorders, especially with atypical or multi-system immune dysfunction. Although not performed in all of our identified patients, genetic testing is considered crucial in identifying and classifying IEI disorders [11].
Traditionally, IEI has been associated with recurrent or severe infections. However, our study highlighted the importance of non-infectious manifestations, such as autoimmune cytopenias, atopy, and lymphoproliferation, as early indicators of IEI. Regarding non-infectious warning signs, this study showed that hepatosplenomegaly was the most frequent presentation for IEI cases. Eczema, autoimmune hemolysis, lymphadenopathy, and failure to thrive were equally represented in our cohort. This emphasizes that hematological, dermatological, developmental, inflammatory, and chronic illness features among children with autoimmune disorders could raise the suspicion index for IEI disorders. These findings are consistent with Schiavo et al. [9], who identified splenomegaly and lymphadenopathy as frequent signs of IEI, and Al-Herz et al. [12], who reported skin manifestations in 40.3% of IEI patients. On the other hand, 13.6% of IEI patients had none of these clinical abnormalities on examination, imposing a critical finding that normal physical examination does not exclude underlying immunodeficiencies. This indicates that infectious signs in terms of severity or frequency, or family history of IEI, could be the only presentation for IEI [13]. A retrospective study on 2,183 patients from the French national PID registry showed that the risk of autoimmune cytopenia was 120 times higher compared to healthy populations. The study found that autoimmune and inflammatory features were observed among 26.2% of patients with IEI [14]. Another European study by Blazina et al. included 247 patients with IEI, of whom 78% were children. Non-infectious features were evident in 29% of patients [15]. Therefore, our study complemented the existing literature in highlighting the relatively high prevalence of non-infectious manifestations among patients with IEI, including immune dysregulation features, such as autoimmunity and lymphoproliferation. In addition, the heterogeneity of our population showed that multiple IEIs can present with overlapping manifestations, such as organomegaly or autoimmunity features. This mandates careful immunological evaluation and genetic testing to reach accurate diagnoses [11].
Laboratory investigations were conducted in our study to confirm the diagnosis and understand the laboratory pattern of IEI. The diverse immunoglobulin levels reflected the broad variability of immune profiles among IEI patients. Khan et al. believed that IEI should be suspected in patients with elevated IgE levels [16]. Our study showed a wide variability in IgE levels, with a high mean IgE level and ranges reaching 2,500 IU/mL. There was also a wide range in IgG levels among our population, which could be due to different IEI pathophysiologies, where some patients could have immunodeficiencies affecting cellular and humoral immunity, while others could be due to congenital phagocytic defects and combined immunodeficiency. On the other hand, IgA and IgM were within normal to low ranges, which is consistent with previous studies that showed low or normal levels in most IEI patients [17,18,19].
Additionally, our study used flow cytometry to understand the immunophenotyping pattern of patients with IEI. CD markers are important in classifying IEIs levels, and their levels depend entirely on the disease and its pathophysiology [20]. For instance, ALPS is characterized by expanded double-negative T-cells [21]. DOCK8 deficiency is a combined immunodeficiency that shows reduced levels of circulating naive CD8 + T-cells with elevated IgE levels [22]. CVID could be suspected with hypogammaglobulinemia, low CD4 + T-cell levels, and low or absent CD19 B-cell expression [23]. Ataxia telangiectasia is also characterized by reduced levels of CD3 + T-cells, including naive CD4 + T-cells and CD8 + T-cells, and low levels of IgA, IgG2, and IgE [24]. Although other IEI disorders are not characterized by specific CD marker profiles, immunophenotyping could help in understanding their disease pathology, guide in genetic testing, and provide the proper treatment. In our study, laboratory investigations revealed reduced CD19 and CD56 levels in confirmed IEI cases, indicating B-cell and NK-cell dysfunction. These findings are partially consistent with Arumugakani et al., who reported reduced CD4 and CD19 counts in IEI patients [25]. However, our results contrast with Schiavo et al., who observed elevated CD19 levels in some IEI subtypes [9]. These discrepancies may reflect the heterogeneity of IEI and the need for subtype-specific immunological profiling.
Similarly, assessing complement proteins, such as C3 and C4, could help in the early identification of underlying immune deficiencies in IEI children with autoimmunity. However, it is uncommon for IEI to affect the complement system [26]. This was a main observation in our study, where C3, C4, and CH50 levels were mostly within normal ranges. Finally, our study assessed the frequency of autoimmune hemolysis, with positive direct and indirect Coombs tests in 18.2% and 9.1%, respectively. This is consistent with the increasing association between IEI and autoimmune hemolytic anemia. A French study found that 16% of children with autoimmune hemolytic anemia had IEI disorders [27]. Our laboratory results helped further understand the disease characteristics of IEI in children that could guide physicians in the diagnosis and treatment of these disorders.
Our study identified significant correlations between non-infectious signs and confirmed IEI cases. Hepatosplenomegaly showed the strongest correlation (r = 0.67, p < 0.001), particularly in patients with ALPS and CVID. This finding underscores the role of hepatosplenomegaly as a key clinical marker for IEI, consistent with previous reports [1, 2]. Lymphadenopathy (r = 0.52, p = 0.01) and eczema (r = 0.48, p = 0.02) were also significantly associated with IEI, particularly in DOCK8 deficiency and WAS. These correlations highlight the importance of considering IEI in children presenting with unexplained lymphoproliferation or atopic dermatitis [3, 28]. Additionally, failure to thrive (r = 0.61, p = 0.001) and autoimmune cytopenias (r = 0.56, p = 0.005) were strongly linked to IEI, particularly in LRBA deficiency and CVID. These findings align with Cunningham-Rundles et al., who emphasized the association between autoimmune cytopenias and IEI [29]. This also aligned with the study by Zama et al., where between 36 and 64% of patients with autoimmune cytopenias had IEI, indicating the importance of multidisciplinary communication among hematologists and immunologists to improve diagnosis and enhance management [30].
Early and accurate diagnosis of IEI is essential for tailoring the most suitable management according to the specific subtype. Recent targeted therapies have emerged in multiple disorders. In ALPS, sirolimus is effective in controlling lymphoproliferation and autoimmune cytopenias [31]. On the other hand, DOCK8 deficiency is treated with early hematopoietic stem cell transplantation (HSCT) [32]. Additionally, treatment of CVID involves immunoglobulin replacement and immunosuppressants for autoimmune complications, where abatacept was particularly effective in CVID patients with interstitial lung diseases [33]. Therefore, the need for early and accurate diagnosis is essential to guide therapy and improve long-term outcomes in children with IEI.


Comments (0)