
Remember me

During our study period, and from, 6783 patients attended the reception room; of them, 2149 patients presented to the ED, and 100 pediatric patients presented to the ED with renal affection. Sixty-seven patients were males, the age of patients ranged from 3 days to 156 months, and 36 patients had consanguineous parents (Table 1).
Table 1 Demographic data of the study group and their vitals at time of ED presentationSixty-nine percent of our study group were normotensive; systolic blood pressure index ranged between 0.47 and 1.91, with mean ± SD of 1.09 ± 0.28, and diastolic blood pressure index ranged from 0.41 to 1.76, with mean ± SD of 1.02 ± 0.22 (Table 1).
Glomerulopathy patients (n = 46) presented mainly with oliguria (69.5%) followed by nausea and vomiting (47.8%); hemolytic uremic syndrome (HUS) patients also presented with oliguria (81.8%), nausea, vomiting, and hematuria in 72.7% for each; tubular disorder patients (n = 5) included three Barter syndrome patients and two renal tubular acidosis ones; congenital anomalies of the kidney and urinary tract (CAKUT) patients complained of oliguria (72%), fever (64%), and dysuria (64%); and urolithiasis patients presented by pain in 100% of patients, followed by hematuria (85.7%) and oliguria (42.8%) (Fig. 1, Table 2). Convulsions in glomerulopathy patients were mainly due to hypertension in one nephrotic syndrome patient, or as a uremic manifestation with electrolyte imbalance in those with AKI or CKD, while with tubular disorders, convulsions were encountered in two Barter syndrome patients due to hypocalcemia.
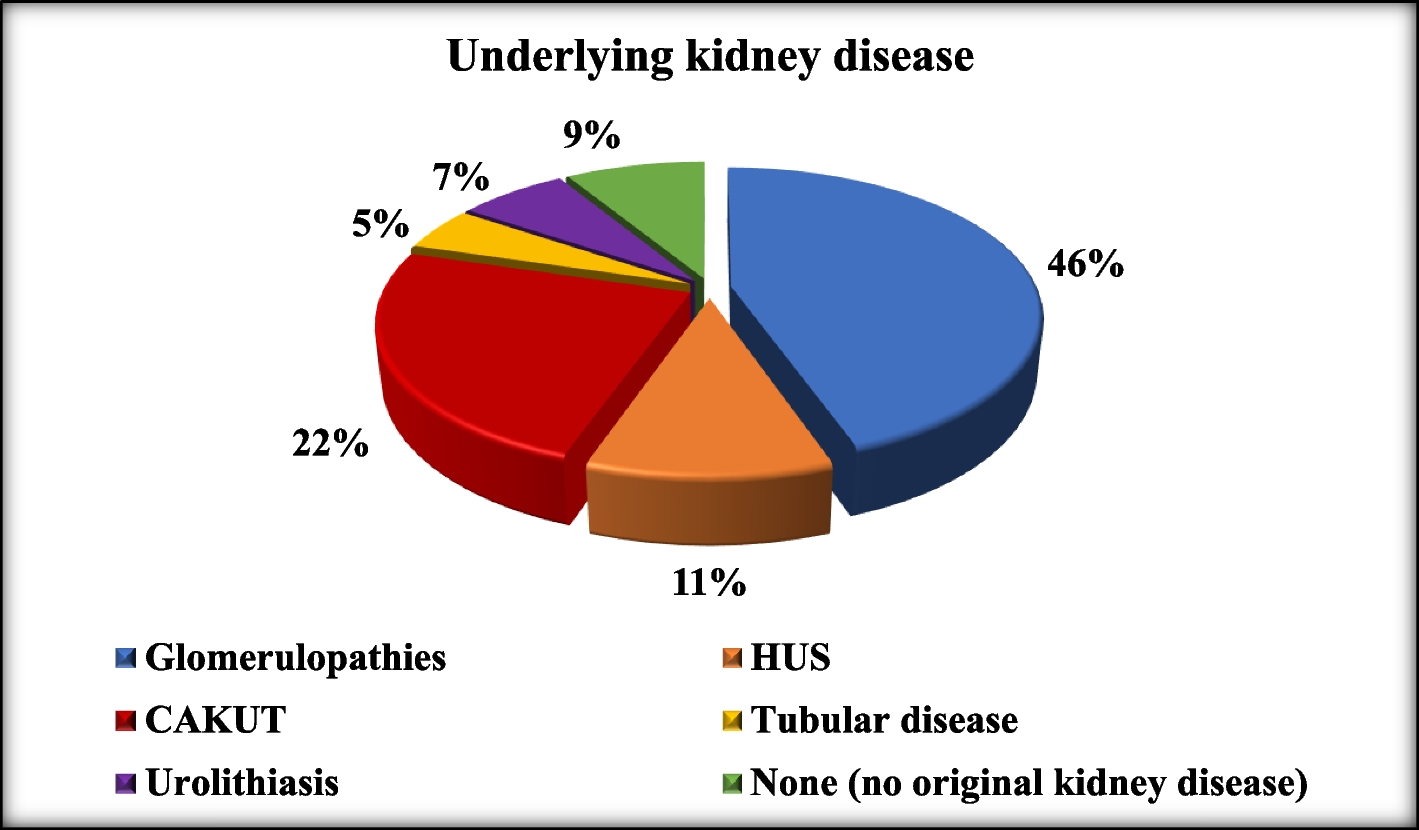
Fig. 1
Pie chart of the underlying kidney disease of patients presenting to the ED in our study. HUS, hemolytic uremic syndrome; CAKUT, congenital anomalies of the kidney and urinary tract
Table 2 Symptomatology of the enrolled patients in relation to their diagnosesPatients presenting to the ED with not previously known original kidney disease (n = 9) but with one or more renal affection symptoms complained mainly of oliguria (55.5%), nausea or vomiting (55.5%), and dehydration (55.5%); in addition, two of them presented with anuria, two with fever, and disturbed conscious level in one patient (Table 2).
Regarding functional diagnosis, 27 patients presented with AKI; most of them were AKI stage I (62.9%) according to the Kidney Disease: Improving Global Outcomes (KDIGO) classification [12], 18 of them had underlying renal diseases, while 9% had multisystem organ affection. On the contrary, 73 patients presented to the ED with CKD, and most of them were CKD stage IIIb (28.7%). Fifty-seven (78%) patients were previously known CKD patients, with 6 of them CKD stages IV–V on regular dialysis and 16 (22%) newly diagnosed as neglected CKD patients. Eighteen of the CKD patients presented with acute symptoms on top on their chronicity, with uremic manifestations due to either failed supportive therapeutic CKD management or missed dialysis sessions in patients who are on regular dialysis (Table 3).
Table 3 Diagnosis vs functional status of the study groupUrine analysis was done in 73 out of our 100 patients, 29 patients had pus cells less than 10 (39.7%), and 16 (21.9%) had pus cells over 100. Of our 20 enrolled patients with urinary tract infection (UTI), 18 patients had precipitating factors for renal back pressure changes as posterior urethral valve (PUV) (75%), vasico-ureteric reflux (VUR) (15%), and pelvi-ureteric junction obstruction (PUJO) (10%). All of the UTI patients presented with fever (100%), many presented with pain (65%) and dysuria (60%), and some had anorexia (40%). Positive urine cultures showed resistant Klebsiella (40%), Pseudomonas aeruginosa (30%), and Escherichia coli (30%), which were only sensitive to polymyxin (11%), amikacin (9%), and gentamicin (7%).
Management of our patients presenting to the ED with renal affection included different modalities, and all patients (100%) received conservative management in the form of monitoring their vitals, their urine output, and correction of dehydration, monitoring their electrolytes, and, when needed electrolytes correction, receiving antibiotics and antihypertensives.
Steroids were needed in 12 patients, 8 with nephrotic syndrome, 1 new case and 7 relapsing disease, and 4 other patients with impaired kidney functions, oliguria, and persistent hematuria due to acute glomerulonephritis.
Twenty-one patient received dialysis: 14 of them had peritoneal dialysis (PD), 6 patients had hemodialysis (HD), and 1 steroid-resistant nephrotic syndrome patient had continuous renal replacement therapy (CRRT) session. In addition, plasmapheresis was needed in one newly diagnosed case of atypical HUS.
Out of our 100 cases encountered, 2 patients were discharged to home, 74 patients needed inward admission, and 24 patients were admitted at NICU/PICU. Mortality was encountered in only 2% due to severe sepsis and associated multiple organ system failure from those admitted to PICU/NICU (Fig. 2).
Fig. 2
The emergency department outcome of the study group
Comments (0)