ROP is one of the main causes of childhood blindness globally. Its incidence varies from one country to another, reflecting differences in economic levels, screening guidelines, and perinatal care levels [11].
Many risk factors were found to predispose to ROP. In this study, low BW was an independent risk factor for ROP, which is consistent with other studies [2, 12].
ROP frequently occurs in combination with other newborn morbidities [13]. Similar to previous studies [12, 14], we found that BPD incidence was statistically higher in patients with TR-ROP. Moreover, a significantly large proportion of the patients who developed TR-ROP received surfactant therapy and had a longer duration of assisted ventilation and oxygen therapy suggesting a severe respiratory distress syndrome which resulted in subsequent BPD. Both ROP and BPD share a common pathogenesis which is abnormal vascularization [14].
Additionally, there was an association between IVH and TR-ROP, which agrees with other studies [15, 16]. IVH follows the rupture of the immature, fragile subependymal capillaries due to decreased cerebral perfusion and hypoxia. Therefore, tissue ischemia and vascular immaturity are characteristics shared by both ROP and IVH [17]. Patients who developed TR-ROP had a higher incidence of NEC. Recently, Zang et al. [18] reported that early intestinal environment had a role in the pathogenesis of ROP suggesting the presence of a gut-retina axis as a result of the dysregulation of VEGF and IGF-1.
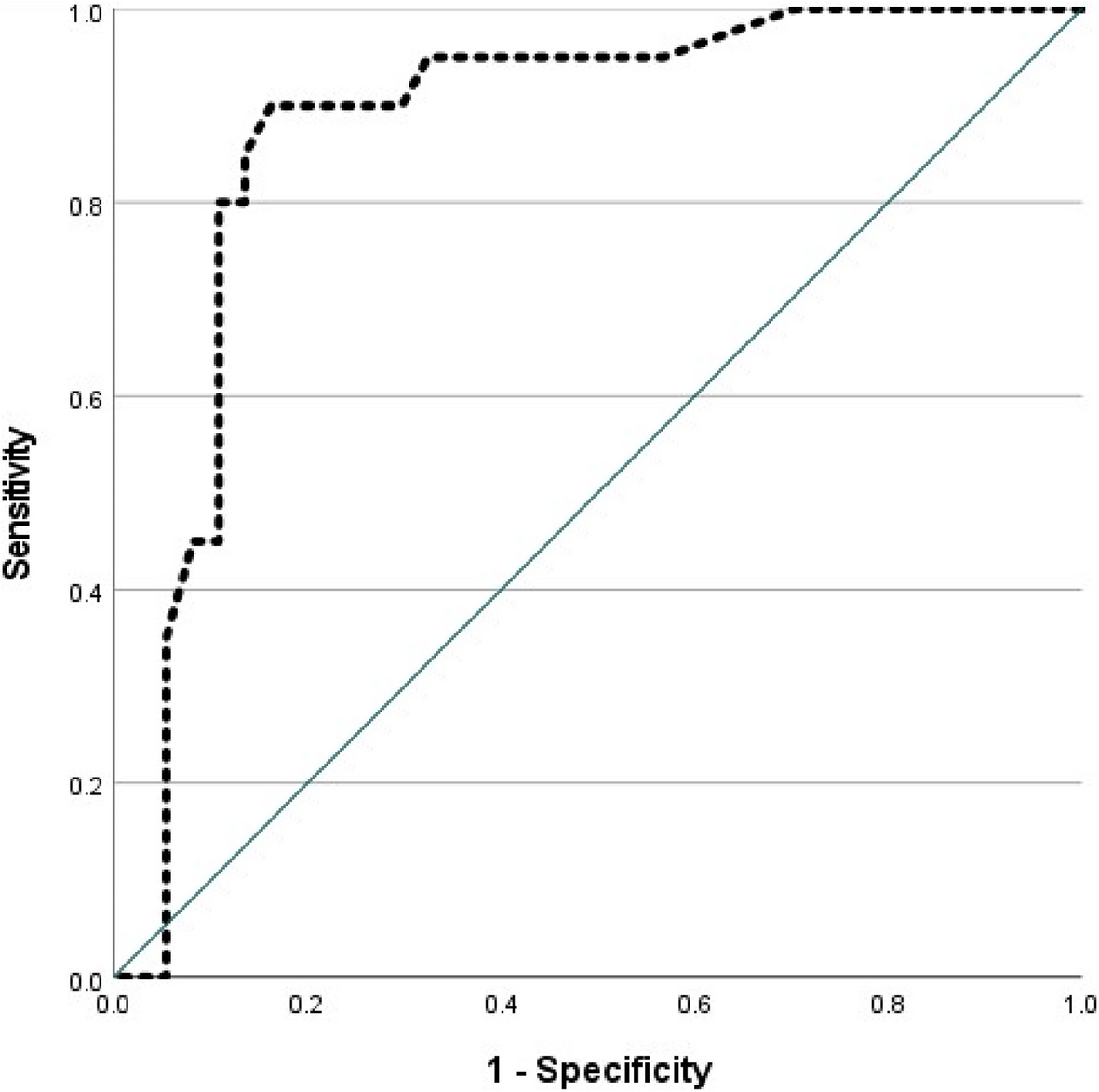
It is possible to detect neonates who are at risk of developing TR-ROP using predictive algorithms [19]. In a sample of 474 Brazilian infants, ROPScore exhibited a sensitivity of 98% and a specificity of 56% for predicting TR-ROP, assuming a particular cut-off level of 14.5 [6]. Similarly, this study found that ROPScore had 100% sensitivity and 67.9% specificity for predicting TR-ROP at a cut-off point of 14.6. According to our study’s NPV calculation, there was a 0% chance that a preterm newborn with a ROPScore below the cut-off point (14.6) would develop TR-ROP. Likewise, Cagliari et al. [20] and Lucio et al. [21] reported similar NPV and PPV with cut-off points of 14.5 and 16.6, respectively. Therefore, patients with those higher scores should undergo more evaluations.
ROPScore is generated by inserting the weight at the 6th week of life. The early hospital discharge of well-improved infants poses a challenge that they could be missed [22]. Due to these challenges, we applied the ROPScore at week 2 and week 4 of life by inserting the proportional weight gain at the 2nd and the 4th postnatal weeks, respectively, into the equation and calculated the cut-off point. The cut-off values of the ROPScore at weeks 2, 4, and 6 of life for predicting TR-ROP were 14.95, 14.55, and 14.6, respectively, with similar sensitivity and specificity. Early calculation of the ROPScore is not intended to replace the current screening recommendations but rather to help early identification of infants at risk through closely observing them.
Moreover, it can reduce the number of stressful eye examinations in those at very low risk for the disease.
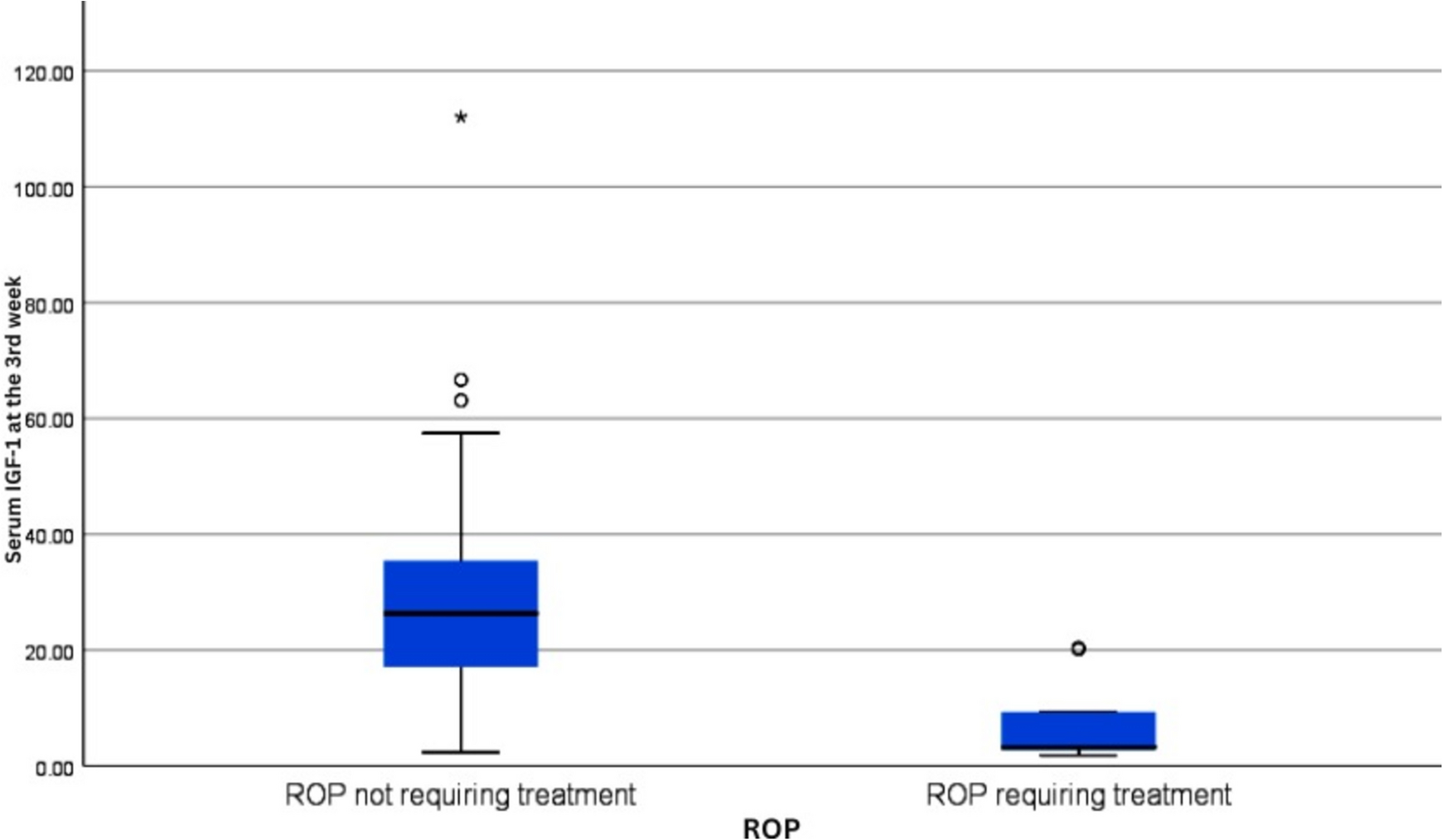
ROP pathogenesis has two important phases: The first phase is after birth, where there is an arrest of retinal vascularization mainly because of low levels of growth factors including IGF-1 that results in retinal hypoxia. In the second phase, the hypoxic retina increases the expression of VEGF that promotes neovascularization [23]. After birth, preterm infants have much lower IGF-1 levels than full-term infants [24]. According to Pérez-Muñuzuri et al. [7], an increase in IGF-1 levels starting from the 3rd to the 5th week of life may contribute to the proliferative phase of the disease. This is why they mentioned that while IGF-1 replacement may be beneficial in the first few weeks of life, it can be potentially hazardous after the third week. In this study, the mean level of serum IGF-1 was statistically noticeably lower in neonates with TR-ROP, despite the relatively small number of infants who developed TR-ROP in this cohort, indicating a significant link between reduced serum IGF-1 level in week 3 of life and the subsequent development of TR- ROP. This aligns with the result by Pérez-Muñuzuri et al. [7]. On the contrary, other studies found no significant difference in serum IGF-1 between infants with and without ROP [25, 26]. A recent meta-analysis by Fu et al. [27] that included 912 neonates concluded that low IGF-1 level at post-menstrual age 33–36 weeks is a significant risk factor for ROP, which is quite consistent with our results. Given the role of IGF-1 in ROP, monitoring its levels would help in diagnosis and treatment of ROP.
We assessed weight gain and proportional weight gain at weeks 2, 4, and 6 as indicators of the nutritional status of the babies. We found a statistically significant higher birth weight in patients with mild ROP not requiring treatment than those with severe TR-ROP (p 0.01). However, the mean weight gain, as well as the mean proportional weight gain at the 2nd, 4th, and 6th weeks of life, were not significantly different between both groups (p 0.68, 0.326, and 0.939, respectively) and (p-value 0.358, 0.154, and 0.514, respectively). This is similar to Sute et al. [28]. Serum IGF-1 may be more accurate in predicting ROP as weight gain may be non-physiological due to other preterm infants’ morbidities such as excessive edema due to sepsis or hydrocephalus [29]. Assessing the nutritional history in detail may have helped better explore the relation between nutritional intake, serum IGFF-1, and ROP. Recently, parenteral administration of amino acids and lipids along with feeding breast milk has been shown to play a significant protective role against ROP [30].
Given the higher incidence of ROP in LMIC as is the case with Egypt with special emphasis on crowded rural areas [31] where the health care facilities are burdened, utilizing ROP score and serum IGF-1 prioritizes high-risk infants for screening by trained ophthalmologists. ROP score can be easily calculated through accessible clinical data, while IGF-1 testing can be included in routine blood work of preterm infants at risk. As regards feasibility, training neonatologists on how to calculate the score and IGF-1 sampling together with partnerships with university hospitals on standardizing IGF-1 sampling paves the way to never missing a high-risk premature. Creating clear referral pathways for infants ensures they receive timely intervention improving overall outcome while properly allocating scarce resources to those who need them the most. Overall, this will lead to a reduction in blindness. In addition, ROP management at the early stage is less complex and costly than in the advanced stages.
Limitations
Some potential limitations should be noted. First, this study had a small sample size. Second, the ROPScore model may overlook aggressive posterior ROP cases with very early and rapid progression. Lastly, the ROPScore included preterm infants of ≤ 30 weeks and/or ≤ 1500 g. However, older and larger infants may also have TR-ROP, especially in LMICs [32].


Comments (0)