This cross-sectional study was performed on preterm neonates to assess platelet indices’ ability to predict the hemodynamic significance of PDA and found that PDW was the only independent predictor of hsPDA, in addition to the clinical Kindler scoring system. Yet, the echocardiography examination remains the most reliable method for diagnosing hsPDA.
In our study, all echocardiographic parameters used for definitive diagnosis of hsPDA were considerably different between both groups, p < 0.001. Left atrium/aortic root ratio of ≥ 1.5 and/or an internal ductal diameter of ≥ 1.5 mm were the most definitive indicators of hsPDA in this study. However, different echocardiographic parameters were used for the diagnosis of hsPDA in other studies, such as left ventricular septal systolic velocity that was identified as a reliable parameter to detect hsPDA [9], increased left ventricular output and end-diastolic velocity of left pulmonary artery greater than 20 cm/s were defined as indicators of hsPDA [22], and retrograde declining aorta flow associated with PDA diameter > 1.5 mm was found to be the best indicator of hsPDA [23].
In this study, individual parameters of the Kindler score used to screen hsPDA were significantly different between both groups except for respiratory deterioration, hepatomegaly, and increased precordial pulsations. This partially agrees with Kindler et al. study [5], which found that respiratory deterioration, hepatomegaly, tachycardia, and systolic murmur were statistically insignificant between both groups and developed a new short clinical score composed of only four clinical signs (increased precordial pulsations, accentuated femoral pulses, oliguria and metabolic acidosis, and apnea or mechanical ventilation), these four parameters correlated most greatly with the development of hsPDA, confirmed by echocardiography.
Numerous research has investigated the relationship between platelets and hsPDA occurrences among preterm newborns. Platelet reactivity was assessed using MPV and PDW data in addition to platelet counts, and inconsistent results were seen [24].
In this study, on investigating the relation of platelet count and indices to the hemodynamic significance of PDA, only PDW was significantly different between both groups (p = 0.001), being higher in the hsPDA group. MPV and PDW are important indicators of platelet volume, which is intimately linked to platelet function [17, 25]. It has been proposed that compromised platelet function may significantly influence the pathophysiology of ductal patency in prematurity [13]. Consequently, a high MPV denoting a high level of platelet activity, platelet adhesion, and aggregation will result in greater damage and decrement of platelets, and this will encourage the bone marrow to produce more new platelets of all sizes, which will raise PDW. According to some earlier research, premature infants with high MPV and PDW are more likely to develop hsPDA [15, 17]. PDW seems to be a more accurate indicator of platelet activation than MPV because it did not rise following a single platelet distention caused by platelet swelling. Using MPV and PDW combined may improve the accuracy of predicting platelet activation [15, 26].
On the other hand, another study found that there was no significant difference in MPV and PDW between the PDA and non-PDA groups, while low platelet mass index and low RDW to platelet ratio were linked to PDA (p = 0.22 and 0.79, respectively) [24]. In addition, a retrospective investigation of preterm neonates with hsPDA revealed that high platelet mass and MPV were independent risk factors for hsPDA, while platelet count and PDW were not associated with an increased probability of hsPDA closure [16]. Additionally, eight studies that were part of a systematic review and meta-analysis assessed the link between PDW and hsPDA. The results indicated no significant difference in PDW between the hsPDA and the non-hsPDA groups [1].
In this study, although platelet count was noted to be decreased in the hsPDA group than in the non-hsPDA group, it was not significantly different between both groups; this was in line with previous studies [7, 14, 15]. However, in a different study, infants with PDA had greater mean blood CRP and PDW and a significantly lower mean platelet count than infants without PDA (p = 0.04) [27]. It was proposed that this had to do with the combined influence of a single common cause (sepsis, for example) on platelet function and number as well as the failure of PDA closure. The observed correlation could, therefore, be more with infection (especially low-grade infection) and ductal patency than with platelets playing a pathogenic role [28].
Nevertheless, our analysis showed no significant difference in CRP or platelet count between the two groups (p = 0.892 and 0.318, respectively), suggesting that the variation in PDW between the two groups was unrelated to sepsis. Furthermore, the two groups matched well in terms of birth weight, gestational age, and perinatal variables, indicating that the variation in PDW is likely due to hsPDA and unaffected by external variables.
Other hematologic indices, such as RDW to platelet count ratio and PLR, have been previously proposed as markers for hsPDA and treatment response, in addition to MPV, PDW, and platelet mass [7, 12, 29]. However, in our study, there was no significant difference between both groups considering RBC count and related ratios and WBC count, differential, and ratios.
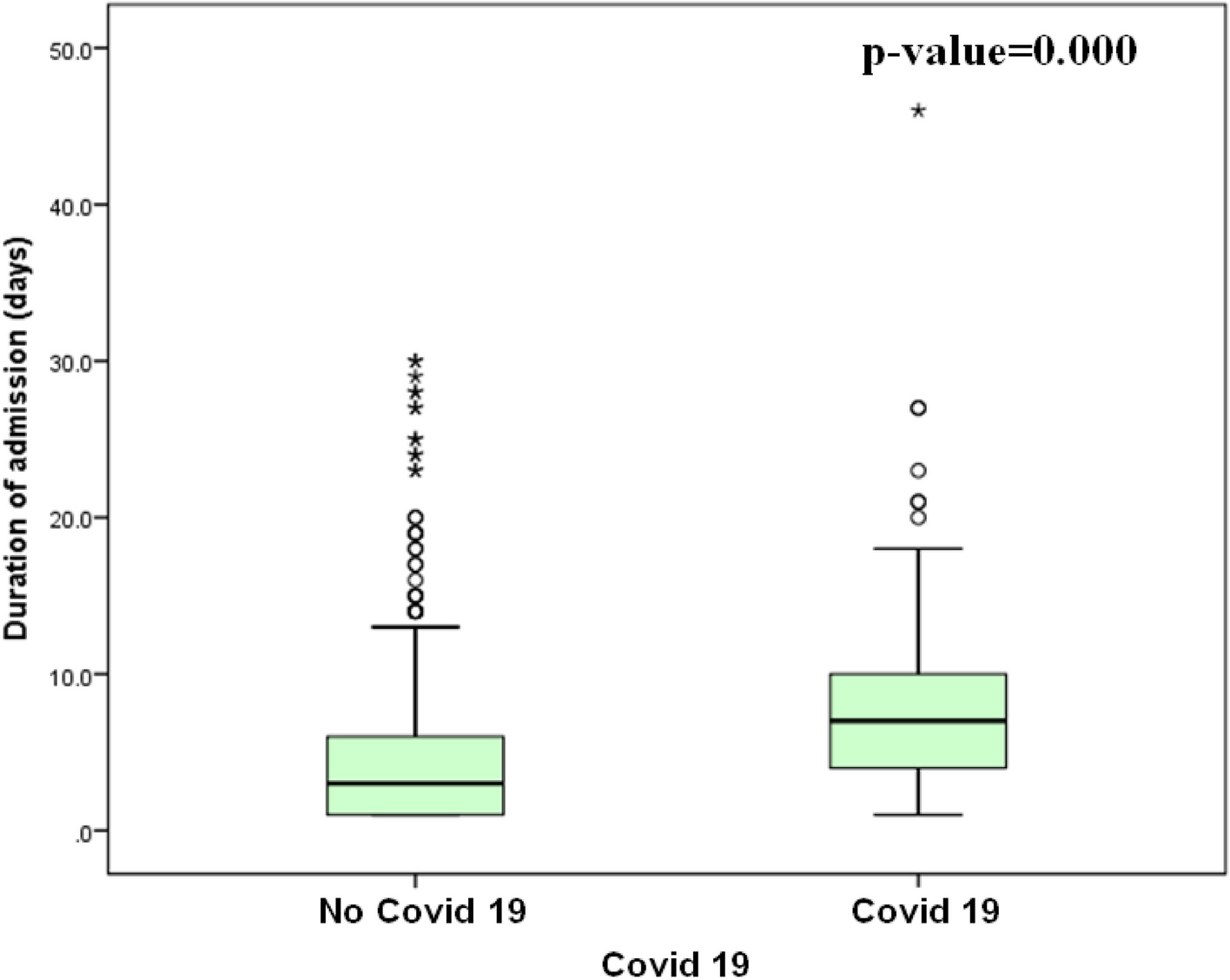
On assessing the outcome of neonates in our study, comorbidities such as worsening respiratory distress, pneumothorax, pulmonary hemorrhage, and increased ventilation requirement were significantly higher in the hsPDA group. Additionally, their hospital admission period was noticeably longer. It has been previously shown that PDA’s impact on systemic and pulmonary blood flow is associated with pulmonary complications and systemic hypoperfusion [15, 24, 30]. The hsPDA group was previously found to require more mechanical ventilation, which led to an increase in hospital stay duration [30, 31].
The CRIB II score was significantly higher (p = 0.001), and the survival rate was significantly lower (p = 0.008) in the hsPDA group than in the non-hsPDA group. This was comparable to other earlier studies [30, 31, 32]. PDA can raise the rates of morbidity and mortality in preterm babies. Consequently, prompt identification and treatment of preterm infants with PDA will enhance clinical results, minimize the need for mechanical ventilation, and decrease hospital stays [10].
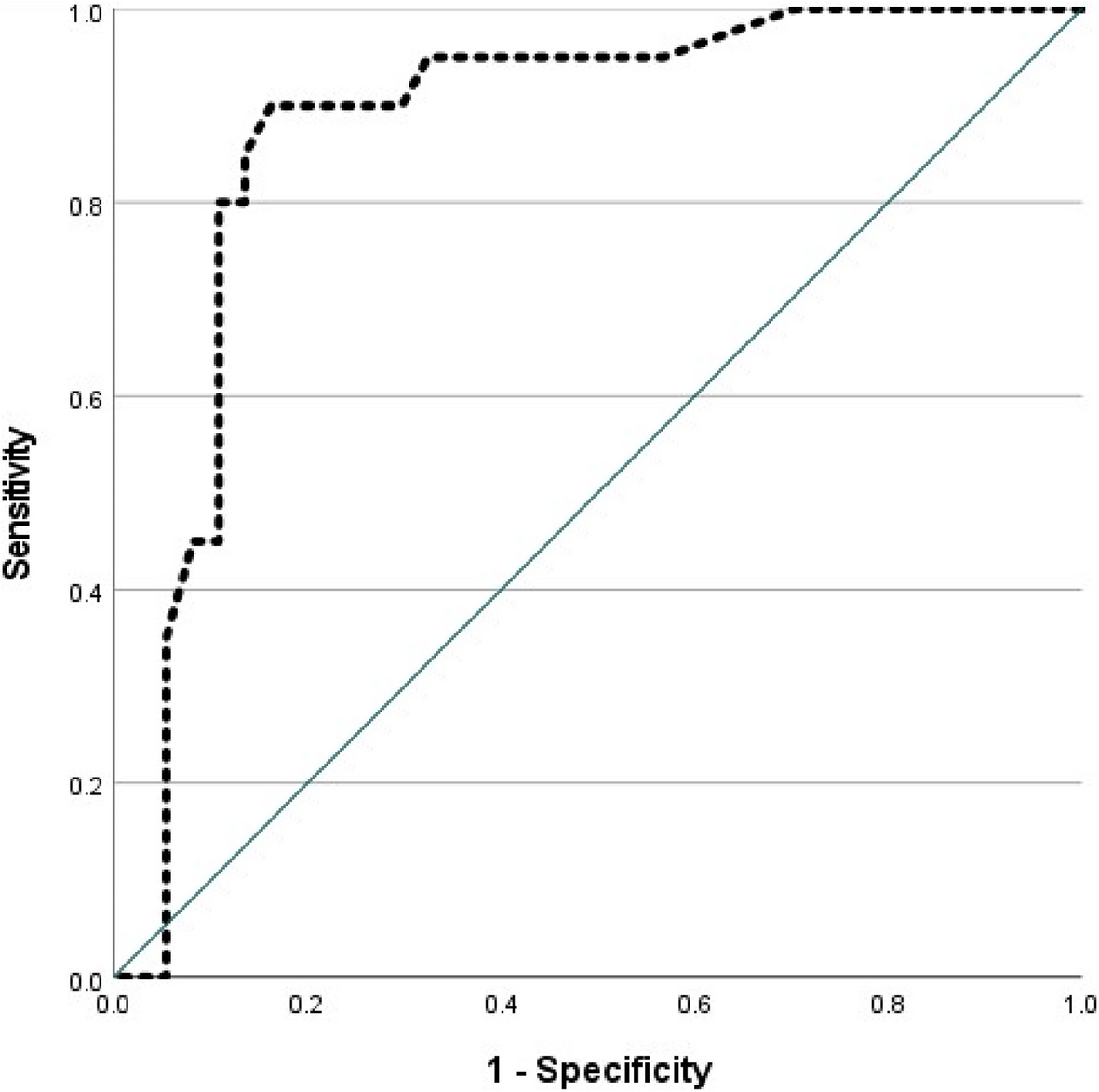
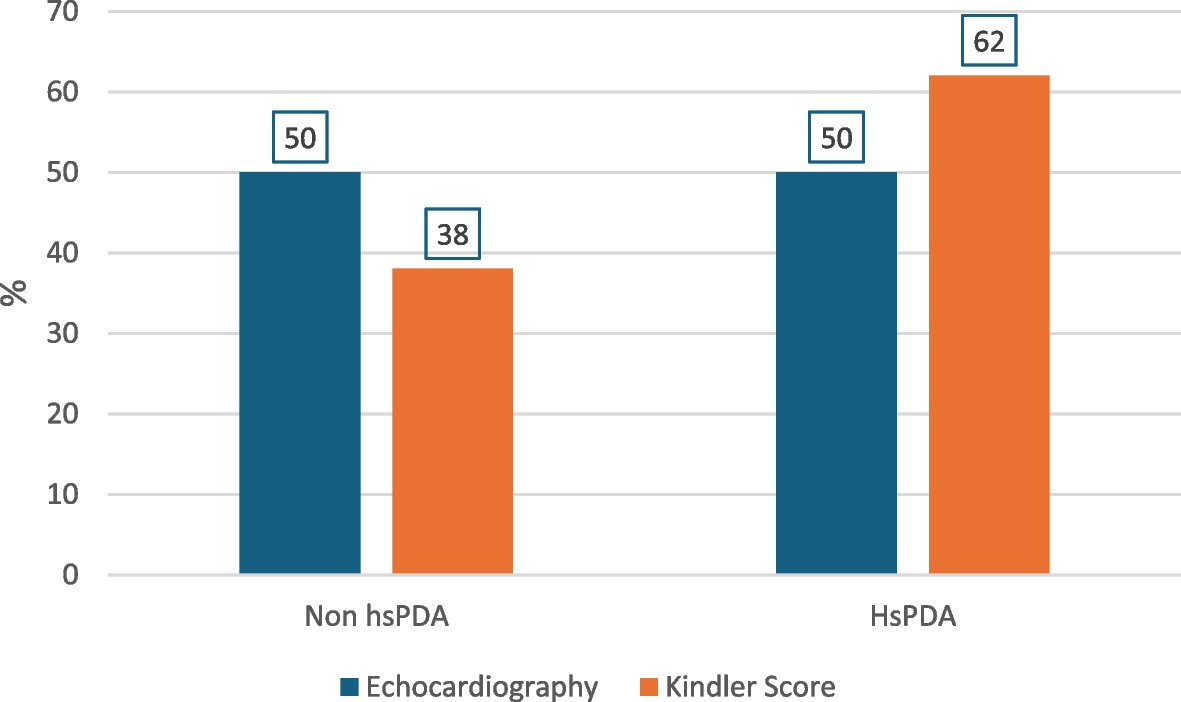
Using ROC curve analysis in the present study, the Kindler scoring system was highly correlated with hsPDA, p < 0.001, with a high sensitivity of 100% and a modest specificity of 56% at a cut-off level of 2.5. Additionally, it was found to be an independent predictor of hsPDA using multivariate logistic regression analysis, p = 0.001. In Kindler et al.’s study, using a cut-off level of 1.5, sensitivity and specificity were 70.6% and 61.5% on day two, respectively, and increased to 88.2% sensitivity and 76.9% specificity on day four [5]. The majority of clinical signs had inadequate sensitivity in the first days of life, according to earlier reports. Hence, clinical diagnosis of PDA has a few days lag as compared to echocardiography [6, 8].
The Kindler scoring system has some limitations, as it cannot discriminate between neonates with non-hsPDA and neonates with no PDA. Moreover, overestimation is one of its drawbacks due to the overlap of its clinical parameters with many other diseases. However, this clinical scoring system did not miss any case of hsPDA, indicating that it is a good screening test for hsPDA, being a non-invasive way to guide the use of the echocardiography and help limit unnecessary exposure of preterm babies to hypothermia and sepsis. Still, echocardiography is the standard diagnostic test to evaluate the hemodynamic significance of the PDA [5, 11].
Using the ROC curve, we found a significant correlation between increased PDW and hsPDA (p < 0.001). Furthermore, PDW demonstrated a high specificity of 72% and an approved sensitivity of 60% at a cut-off value of 18.85fL. Also, combining both RDW and clinical Kindler score augmented its specificity to detect hsPDA cases. Moreover, using multivariate logistic regression analysis, PDW was observed as an independent predictor of hsPDA, p = 0.004. PDW was also considerably higher in the hsPDA group in different research (p = 0.023). At a cut-off value of 11.45fL, PDW showed 65% sensitivity and 66% specificity. Also, using multivariate regression analysis, higher PDW was found to be an independent predictor of hsPDA (p < 0.05). The two groups had no significant difference in platelet count, MPV, platelet mass, or other platelet parameters [15]. Similarly, in another study, high PDW within the first 3 days of life was related to hsPDA, p = 0.003. Multivariate analysis revealed that hsPDA was associated with low platelet count (p = 0.005) and high PDW (> 17 fL) (p = 0.003) [14].
This study is limited by the short follow-up duration. We recommend further investigations with a longer follow-up time. Additionally, we recommend assessing the relation between the platelet indices and the fate of PDA and its response to treatment.


Comments (0)