In this study, we had 45 cases diagnosed as persistent pneumonia which represented 75% of the cases and 15 cases with recurrent pneumonia which represented 25% of the cases with total number 60 cases. This comes in contrary to Hossain et al. [14] where 80% of the cases in their study presented with recurrent pneumonia and 20% presented with persistent pneumonia. This may be attributed to different localities between two studies together with development of persistent infection with different organisms owing to antibiotics abuse and microbial resistance.
In our study, the majority of cases (65%) were males and 35% were females. This comes in agreement with Bolursaz et al. [15] who also found that 55% of cases were males. This may be attributed to the impact of gender impact on immune response [16]
Regarding risk factors in studied group, 20% of patients had history of atopy,recurrent chocking in 13.3%. Ozdemir et al. [17] reported similar findings, identifying asthma as the leading cause of recurrent pneumonia in their study (30.64%), followed by immune disorders (17.75%), aspiration syndromes (17.75%), and congenital abnormalities (16.12%). This could be attributed to atopy as allergic inflammation can suppress the interferon release, increasing a child's susceptibility to infections [18].
In the present study, the main presenting symptom was cough, which was present in all cases followed by fever (78.3% of cases). The main sign was diminished air entry over the affected lung lobe(78.3%) followed by audible adventitious sounds as rhonchi or crepitations (40% of cases).This comes in agreement with Çapanoglu et al., [5] where most common symptoms were cough 95.5%, fever 59.9% and wheezing 47.9%.
CBC showed leukocytosis in 41.7% of our patients with predominant neutrophils in about 68% of them, CRP was positive in thirty-nine patients (65%) and ranged from 0 to 260 mg/L with median 20 mg/L. Similar to our results Esposito and Principi [19] who reported that total leucocytic count was used by clinicians to help in diagnosis of pneumonia, assessing its severity and predicting patient outcome.
BAL analysis revealed that 58.3% had many pus cells. Concerning isolated organism, Bacterial infection was found in 21 patients with commonest organism was Klebsiella (8.3%), followed by Strept. pneumonia (6.8%) while BAL was negative in 37 cases (61.7%),this may be due to prolonged usage of empirical antibiotics before bronchoscopy in these cases, this comes in line with Rhodes et al., [20] who argued that previous administration of antimicrobials will make microorganism detection in cultures a difficult task, not to mention that cultures have low sensitivity in general compared to more advanced diagnostic techniques [21].
Our study revealed that about 54.5% of patients with positive cultures (bacterial & fungal) had biofilm formation, thus the treatment of chronic lung infections is greatly hindered by the multidrug tolerance caused by biofilm formation [22].
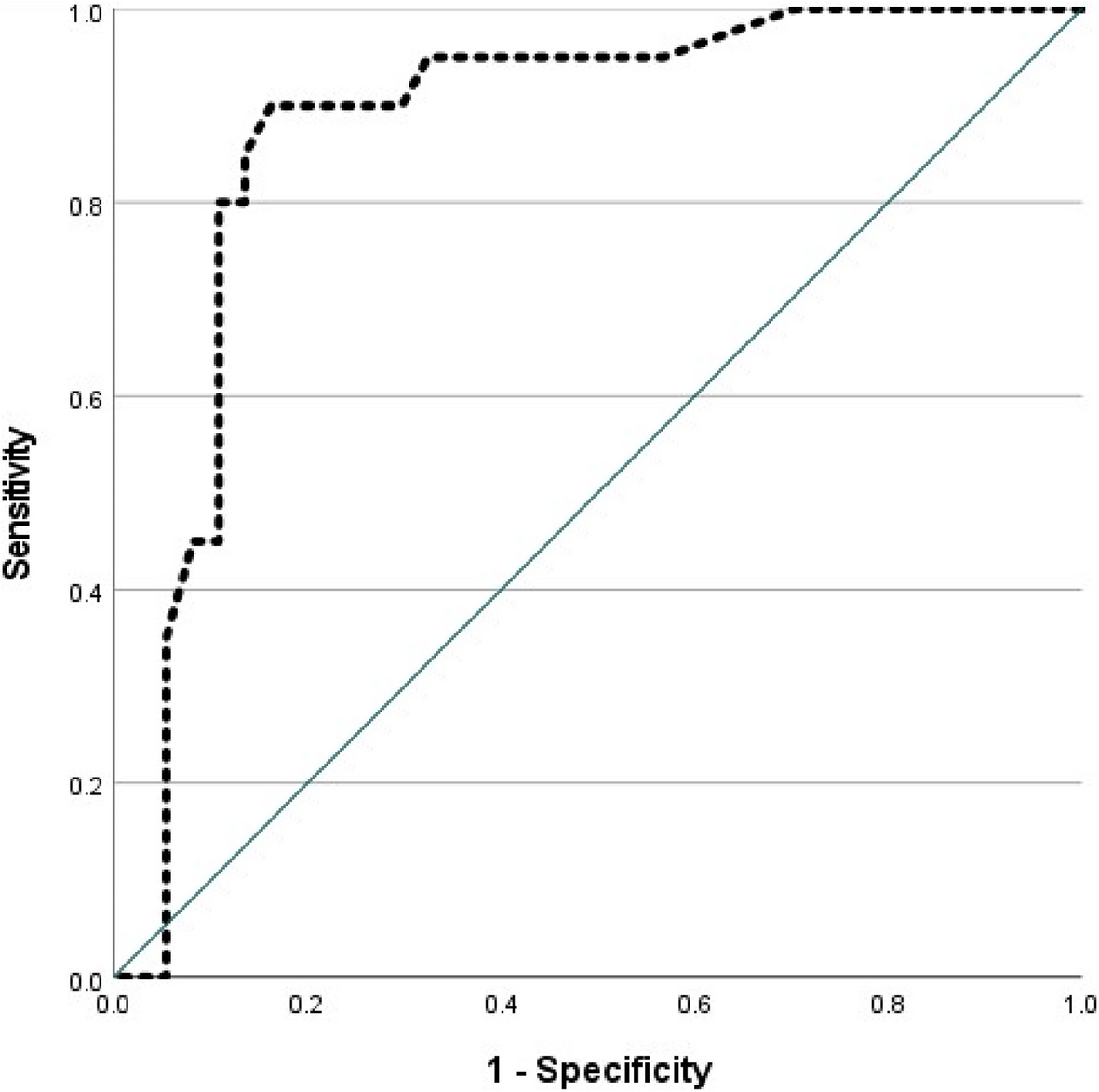
Our study revealed that there is statistically significant relation between presence of bacterial LRTI (positive culture) and TLC in BAL and serum CRP, with the best cutoff value of TLC in BAL in diagnosis of bacterial infection is ≥ 375 with area under curve 0.875, sensitivity 90%, specificity 83.8%, positive predictive value 75%, negative predictive value 93.9% an overall accuracy 86% (p < 0.001). This comes in agreement with Choi et al., [23] who reported that BAL fluid total WBC count showed the best discrimination, with an area under the curve of 0.855 (95% CI, 0.750–0.960). BAL fluid total WBC count ≥ 510/µL had a sensitivity of 83.3%, specificity of 78.3%, positive likelihood ratio (PLR) of 3.83, and negative likelihood ratio (NLR) of 0.21.
On the other hand, there is statistically non-significant relation between presence of bacterial LRTI (positive culture) and HBP as both groups had comparable HBP levels and this may denotes presence of bacterial infection in cases with culture negative results, which can be attributed to either prolonged antibiotic therapy, false negative culture (traditional method) or presence of atypical organisms. Thus, real-time PCR may solve this dilemma as it was found to be significantly more sensitive than culture in identifying pathogens in pediatric empyema, in both pleural fluid (79.7% versus 12.5%) and blood (17.8% versus 7.4%) [24].
In contrary to our results, Huang et al., [25] found high HBP values in lavage fluids in those pediatric cases with bacterial pneumonia. Ideal cutoff of HBP in lavage fluid rests at 74.05 ng/mL in that study, for predicting bacterial pneumonia. Discrepancies could be attributed to sample size, comorbidities, microorganism, medication history, and measurement technique.
In our study, there is statistically significant positive correlation between TLC in BAL and CRP (p < 0.001),with statistically significant relation between leukocytosis and TLC in BAL (p < 0.001), serum CRP (p < 0.001) (significantly higher among patients with positive bacterial culture) and biofilm (P = 0.008), Stolz et al., [26] showed similar results.
In our study, bronchoscopic anatomical abnormalities encountered in 17 patients, a similar study by Ravikumar et al., [27] reported that tracheomalacia and tracheal stenosis were the most common finding.
Pierre Goussard [28] also performed a study from national survey which aimed to detect causes of wheeze as wheezing considered to be most common symptom and sign in early childhood and they found that (33%) of study population had anatomical abnormalities that led to wheezing. This included tracheomalacia, bronchomalacia, vascular rings and airway compression by a vascular structure and that is nearly the same in our study.
We found that flexible bronchoscopy could detect an underlying cause in 40% of the patients who had unexplained persistent or recurrent pneumonia, also our study revealed that 58.3% of cases did not match previous diagnosis suspected by clinical and non invasive tests as shown in Table 6, Yavuz et al. [29] showed similar results at who reported that bronchoscopy confirmed the suspected diagnosis in 89% of cases and led to a change in management in 54% of patients. This underscores the utility of bronchoscopy in diagnosing and managing pediatric respiratory conditions.
Table 6 Distribution of the studied patients according to diagnostic value of bronchoscopy with their proportion for the causes of persistent and recurrent LRTI, diagnosis matching pre and post bronchoscopyIn a study by Viyeresegran et al. [30] on unresolved atelectasis in infants, bronchoscopy revealed similar causes, which were congenital anomalies (46.4%), mucus plugs (28.5%), hypoplasia (4%), granulation tissue (3.5%), and foreign body (3.5%).
Similarly, congenital airway anomalies (15%) were the leading causes of persistent and recurrent pneumonia in children in this work. These findings come in line with Little et al., [31] who reported that children with congenital anomalies of the airways (e.g., tracheo-oesophageal fistula or tracheal bronchus) are at increased risk of recurrent or persistent respiratory infections.
Boogaard et al., [32] stated recurrent LRTI in 63% of study population with primary airway malacia. We detected malacia disorders in 3.3% of the cases, resulting in airway collapse, cough, stridor, recurrent and persistent wheezing, and infections. This difference in percentage of malacia disorders may be attributed to studied age group and relatively smaller sample size in comparison to that study.
Our study revealed that six patients (10%) had clear history of foreign body aspiration while 26.7% had doubtful history that necessitated bronchoscopic evaluation as young children are particularly at risk for foreign body aspiration. One study showed that the mean age of aspiration was 24 months with 98% of cases involving children < 5 of age [33].
Patients with neglected foreign body may present with persistent/ recurrent pneumonia. Selection of appropriate bronchoscopy approach, i.e., rigid vs flexible, depends largely on clinical scenario. Rigid bronchoscopy fits patients with a clear history (of foreign body aspiration), or if there is unilaterally diminished air entry, obstructive emphysema, or atelectasis. Flexible bronchoscopy, on the other hand, is the preferred procedure if the history is not clear enough. Classic history of aspiration is not present in up to half patients with history of foreign body aspiration [34].
In our study, foreign body aspiration was present in 8.3% of studied cases, the triad of acute onset of cough, wheeze and decreased breath sound should direct to a diagnosis of foreign body aspiration. These symptoms may be misdiagnosed as bronchitis, asthma or pneumonia and the patients treated with antibiotics, bronchodilators, and corticosteroids which itself lead to alterations in the clinical features and long-term nature of the disease [35].
Flexible bronchoscopy in children is a safe procedure in cases with non-resolving pneumonia or recurrent pneumonia. Minor complications were observed in 16.6% of cases. The most frequent complication was transient hypoxia (10.8%), followed by bronchospasm (3.3%), then cough (3.3%). This agrees with Terkawi et al., [36] who noted that the procedure of the flexible bronchoscopy was associated with transient desaturation, cough, bleeding in the mid airway as well as airway spasm.


Comments (0)