Clinical study design and participants
This was a 12-week, non-blinded randomized controlled trial among the elderly T2DM patients with sarcopenic obesity. The study was approved by the Shanghai Jiaotong University School of Medicine, Renji Hospital Ethics Committee (Approval No. LY2022-039-A), performed in accordance with the Declaration of Helsinki, and was registered with the Chinese Clinical Trial Registry (ChiCTR2200065362). All participants provided written informed consent.
The inclusion criteria for the study population were as follows: (1) meeting the diagnostic criteria for type 2 diabetes mellitus; (2) HbA1c < 7.5% (this threshold was selected in accordance with the safety parameters established in the Guideline for the Prevention and Treatment of Diabetes Mellitus in China [17], and does not necessitate immediate pharmacological intervention) and no use of any glucose-lowering medications (including insulin sensitizer such as metformin, thiazolidinediones; insulin secretagogues such as sulfonylureas, glinides; alpha-glucosidase inhibitors; sodium-glucose co-transporter 2 inhibitors; incretin-based therapies such as glucagon-like peptide-1 receptor agonists, dipeptidyl peptidase-4 inhibitors; insulin) within the past three months (to eliminate pharmacological confounding of intervention effects); (3) age between 60 and 75 years, without gender restriction; (4) sarcopenic obesity, characterized by the presence of both reduced skeletal muscle mass and obesity. The definition of reduced skeletal muscle mass was determined using the skeletal muscle index (SMI) measured through bioelectrical impedance analysis, with a cutoff of < 7.0 kg/m2 for males and < 5.7 kg/m2 for females [13]. Obesity was defined as a percent body fat (PBF) of ≥ 25% for males and ≥ 35% for females [18]. Moreover, subjects with any of the following conditions were excluded from the study: type 1 diabetes or specific types of diabetes; a history of confirmed infection within one week prior to enrollment or at the time of enrollment (including respiratory, urinary, gastrointestinal, or other organ system infections); malignant tumors; rheumatologic or autoimmune diseases; impaired liver function (serum alanine aminotransferase level ≥ 2 times the upper limit of normal); renal insufficiency (creatinine clearance rate < 60 mL/min); heart failure (NYHA class ≥ III); uncontrolled hypertension; history of coronary heart disease; unstable cardiac arrhythmias; severe chronic obstructive pulmonary disease; neuromuscular, rheumatic, or genetic muscle diseases such as myasthenia gravis, dermatomyositis, or Duchenne muscular dystrophy; edema; creatine kinase levels above the upper limit of normal; abnormal thyroid function, including hyperthyroidism and hypothyroidism; use of medications within the past three months that affect blood glucose or muscle (including glucocorticoids, growth hormones, sex hormones, thyroid hormones, niacin, diuretics, phenytoin, gamma interferon, etc.); inability to consume food orally; malabsorption disorders such as inflammatory bowel disease, irritable bowel syndrome, gastrointestinal bleeding, chronic diarrhea, etc.; individuals with ongoing unresolved sports injuries and other conditions unsuitable for exercise, such as a documented history of cervical or lumbar disc herniation, spinal curvature, knee joint injury, diagnosed osteoarthritis, etc.; regular exercisers or individuals with a history of high-intensity exercise, such as fitness enthusiasts, marathon runners, etc.; history of substance abuse; history of alcohol or tobacco dependence; documented history of psychiatric disorders; any other conditions as determined by the researcher that could potentially affect study enrollment.
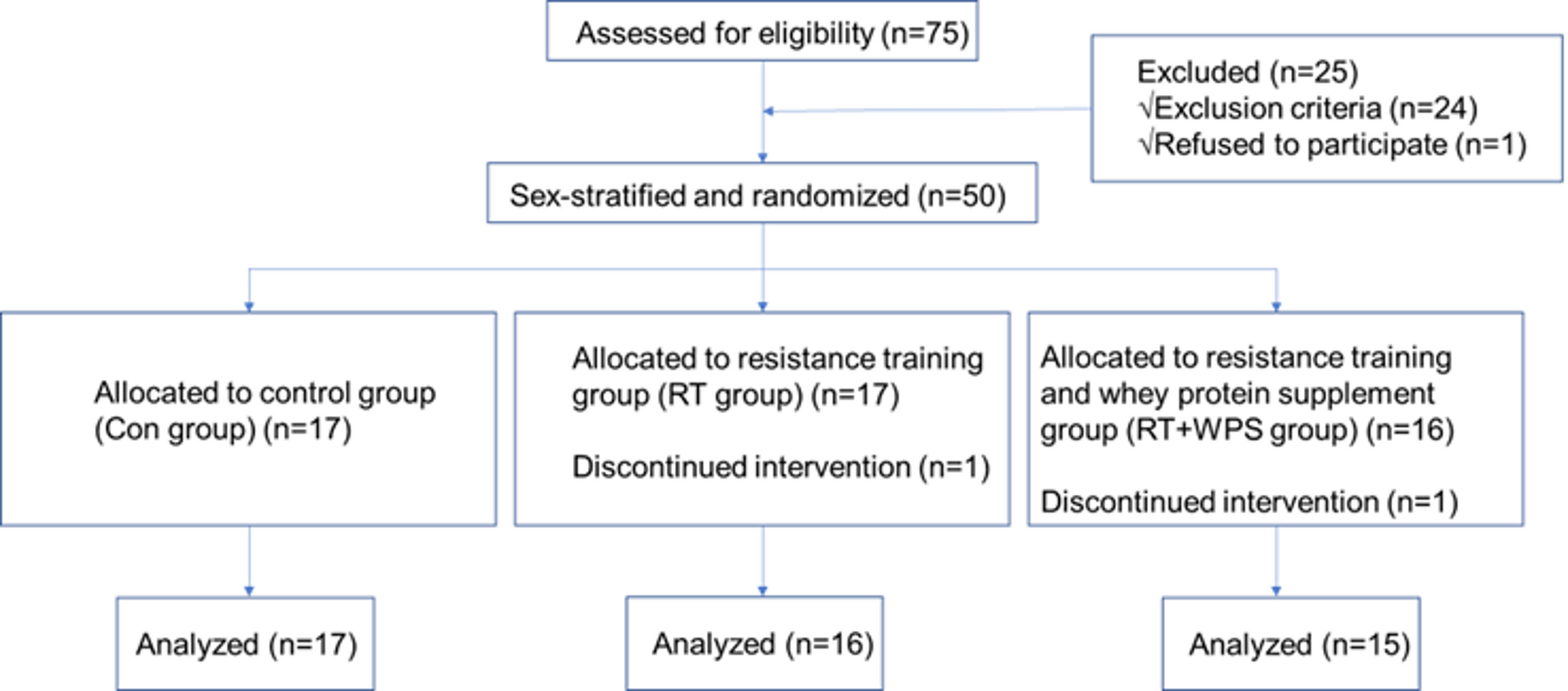
After sex stratification, all the participants were randomly allocated to three groups in a 1:1:1 ratio using a computer-generated random number sequence based on the intervention approach: (a) resistance training (RT) group, which received muscle-building intervention through resistance exercise; (b) resistance training combined with whey protein supplementation (RT + WPS) group, which received muscle-building intervention through resistance exercise combined with whey protein supplementation; (c) control (Con) group, which did not receive any muscle-building intervention. All participants received diabetes-specific dietary education from specialized nurses and were provided with educational handbooks on diet.
Baseline information collection
At baseline, participant characteristics including gender, age, dietary intake, and physical activity level were collected. Dietary intake was assessed through the completion of a 3-day consecutive dietary diary. Participants were instructed to maintain a self-recorded 3-day dietary diary, documenting meal occasions, food items with preparation methods, and food weight (grams). Researchers analyzed daily total energy intake and macronutrient composition (protein, fat, and carbohydrates) using the Booheehealth software, with mean daily intake values derived from the three-day records. Physical activity assessment was conducted by recording daily step counts. Participants wore the Polygon3D electronic pedometer during daily life to record step counts. Data were collected over three consecutive days, and the mean daily step count was calculated from the recorded values.
Interventions
The RT group and the RT + WPS group exercised 2 non-consecutive days per week for 12 weeks. The design of all resistance training movements followed the principles of safety, convenience, efficacy, and suitability for home-based exercise. The following exercises targeted large symmetrical muscle groups: biceps curls, triceps curls, bench press, shoulder press, bent-over rows, squats, deadlifts, and leg swings. Each set consisted of 6 to 12 repetitions. The participants engaged in 2–4 sets of exercise with an inter-set rest duration of 2–3 min. Each session had a 5-minute warm-up and cool-down period. The total duration of each training session was 45 min, with a minimum interval of 48 h between sessions. The intensity was set at 60% of the most recently determined one-repetition maximum, reassessed every 4 weeks.
Within the first month of participant enrollment, a total of three supervised training sessions were conducted on-site to ensure participants’ acquisition of correct exercise techniques. Additionally, one on-site training session was scheduled within the 5th and 9th weeks after the initiation of resistance training. The purpose of these sessions was to modify the exercise program, including exercise modalities, resistance levels, repetition counts, and frequency, based on individual changes in participants’ exercise capacity. This aimed to further optimize the exercise program. During non-site training periods, participants followed the prescribed resistance training program (recorded videos) for home-based training and documented their training completion through online check-ins. Participants were required to complete the resistance training program twice per week. Researchers provided weekly supervision, documentation, and follow-up on participants’ exercise progress via telephone.
The RT + WPS group incorporated whey protein supplementation (20 g/day) into their daily dietary intake. Whey protein was consumed within 30 min after resistance training sessions and during breakfast on non-resistance training days. Researchers also conducted weekly telephone monitoring and follow-up on the participants’ whey protein supplementation regimen.
Outcomes and measurement methods
Blood samples were obtained from each participant’s antecubital vein after an overnight fast at the baseline and the completion of the 12-week intervention period. The primary outcome was the change in glycated hemoglobin (HbA1c) from baseline at 12 weeks, which was assessed using high-performance liquid chromatography (HPLC) method. All participants underwent a 75 g oral glucose tolerance test (OGTT) and an insulin release test (IRT) before and after the 12-week intervention period. The glycemic parameters assessed in this study included fasting plasma glucose (FPG) and OGTT 2-hour plasma glucose (2hPG) which were measured using the glucose oxidase method; and fasting serum insulin (FINS) and 2-hour postprandial serum insulin (2hINS) which were measured using the chemiluminescent method. The insulin resistance indices included the homeostatic model assessment of insulin resistance (HOMA-IR) and the Gutt index, and the calculation formulas could refer to relevant literature [19]. Anthropometric measurements including body height, weight, waist circumference (WC) were measured according to guidelines by the World Health Organization (WHO) [20]. Body mass index (BMI) was calculated as body weight divided by the square of height (kg/m2). Body composition was analyzed using a bioelectrical impedance analysis device (InBody770, InBody, Seoul, Korea). The body composition indices included appendicular skeletal muscle mass (ASM), skeletal muscle index (SMI), body fat mass (BFM), and percent body fat (PBF). SMI was calculated by dividing ASM by the square of height (kg/m2). The muscle function assessment included handgrip strength, which was used to evaluate upper limb muscle strength and was measured by a hydraulic electronic hand dynamometer (Jamar Plus+, Performance Health, USA), and the 5-time chair stand test, which was used to assess lower limb muscle strength. In addition, safety indicators included complete blood count analysis, liver and renal function, creatine kinase levels, and electrocardiography.
Adverse events reporting
Participants were instructed to report any discomfort or injuries during exercise, such as mild muscle or joint pain, skin abrasions, or exercise-related injuries. Additionally, any discomfort arising from whey protein supplementation, primarily gastrointestinal reactions including nausea, vomiting, abdominal pain, bloating, or diarrhea, was to be reported. Furthermore, any abnormalities in safety indicators following the intervention were also to be promptly reported. The researchers would then provide appropriate management and intervention measures in response to these reported adverse events.
Sample size calculation
The sample size calculation was performed using PASS 15 software. The significance level (α) was set at 0.05, and the power (1-β) was set at 80%. The primary outcome of the study was the change in HbA1c. Based on preliminary experimental results, the mean differences before and after intervention were set as 0, -0.3, and − 0.3 for the three groups respectively, with a standard deviation of 0.25. Considering an anticipated dropout rate of 20% in each group, the calculated sample size was determined to be a total of 45 participants, with 15 participants allocated to each group.
Statistical analysis
The normality of distributions of variables was analyzed with the Kolmogorov–Smirnov normality test. Descriptive statistics for continuous variables were presented as mean ± standard deviation (SD) if variables were normally distributed. Group based differences of quantitative variables were compared by analysis of variance (ANOVA) following Turkey’s test for normally distributed data and Kruskal-Wallis H-test for skewed data. Categorical variables were compared by using Pearson’s chi-squared test. The changes in variables were compared among the groups using ANOVA. Correlation analysis was conducted using Pearson’s correlation coefficient. The incidence of adverse events was compared among the groups using Fisher’s exact test. P values < 0.05 were considered statistically significant. All statistical analyses were conducted utilizing SPSS, version 26.0 (SPSS Inc., Chicago, IL, USA).



Comments (0)