
Remember me

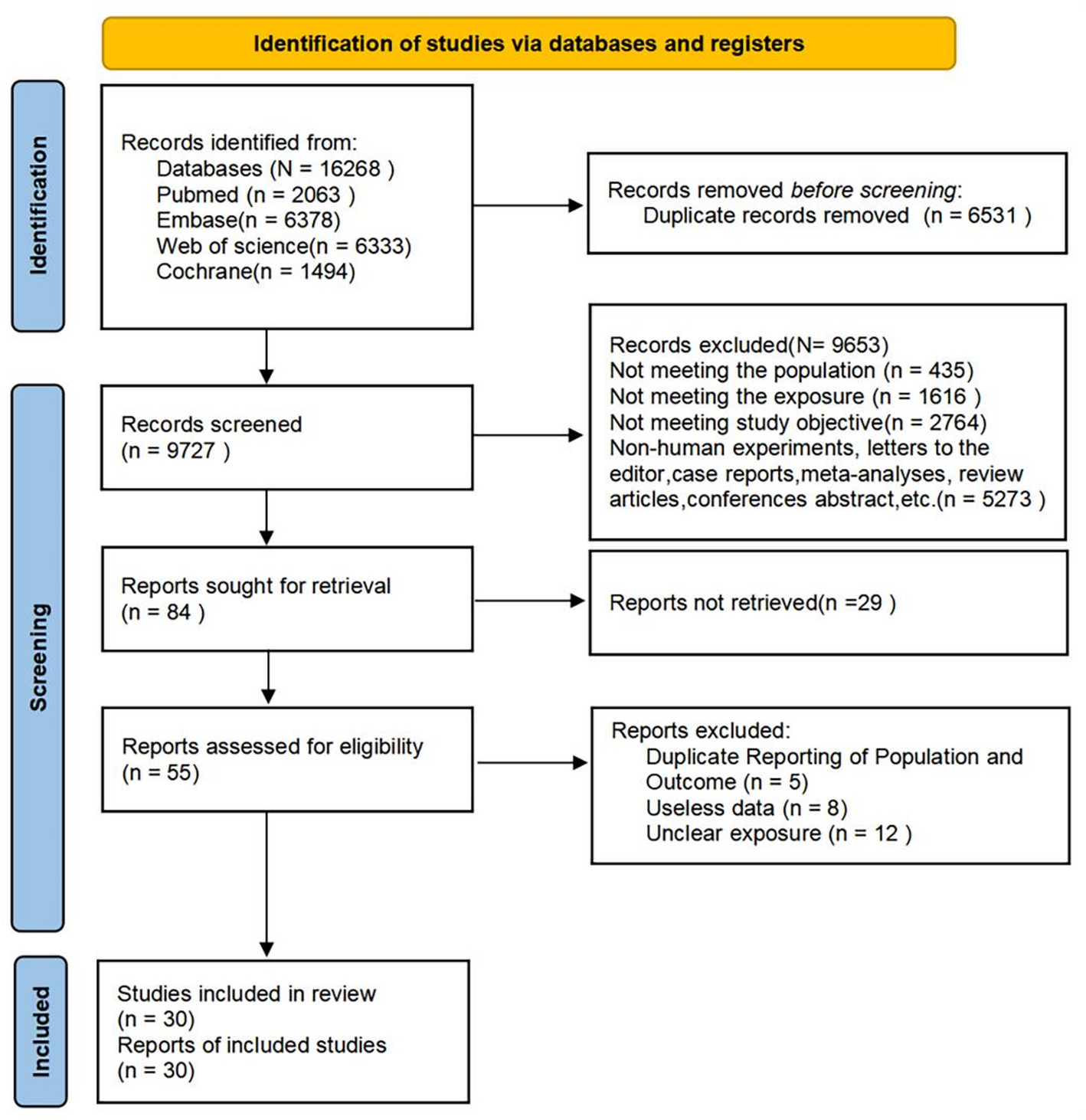


16,268 articles were identified. After excluding 6,531 duplicates, 9,653 articles were eliminated following an initial screening of titles and abstracts. The remaining 84 articles underwent full-text screening, resulting in the exclusion of 54 articles. Ultimately, 30 studies [15,16,17,18, 26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51] were eligible. Figure 1 presents the PRISMA flowchart for literature selection.
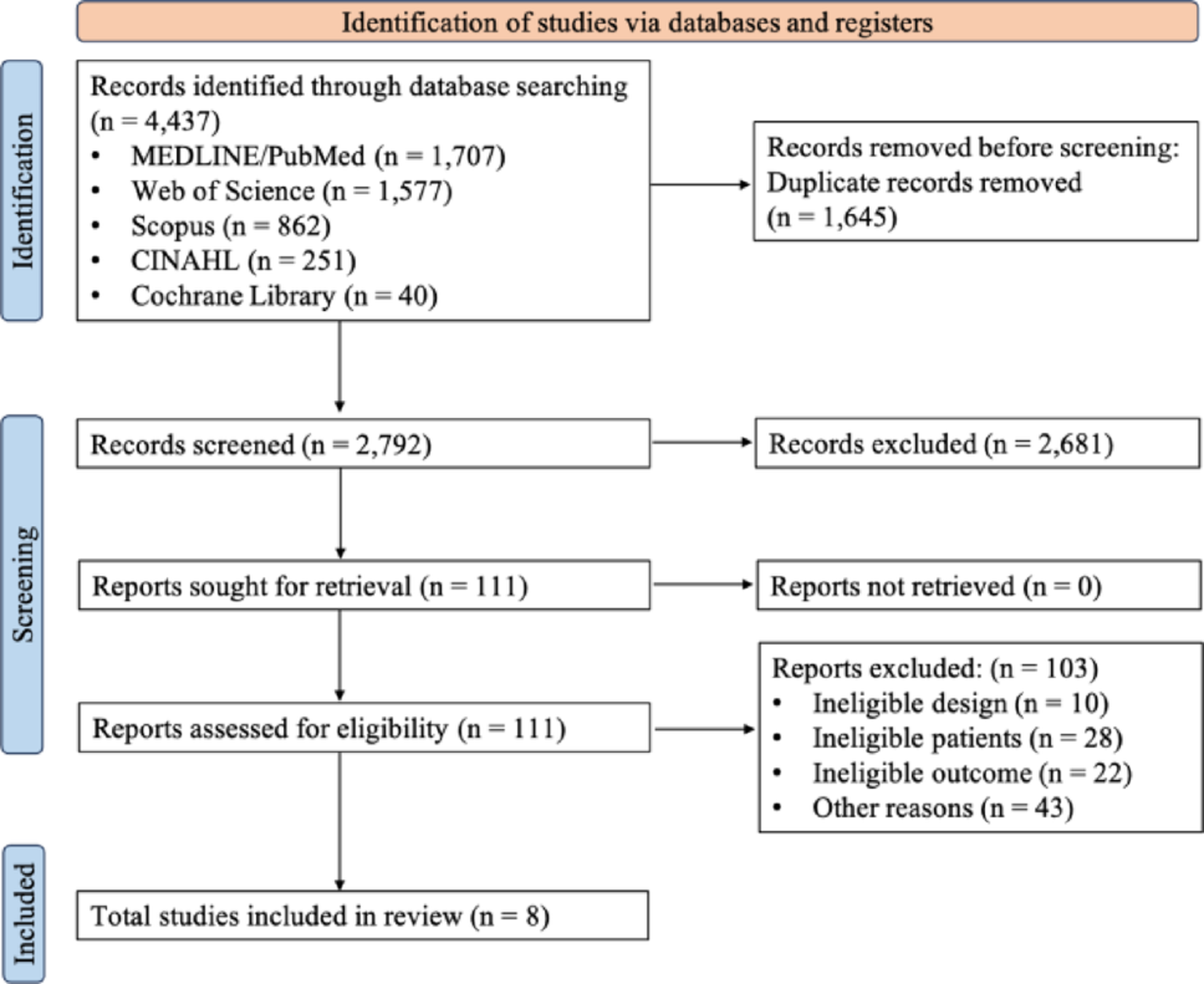
Fig. 1
The PRISMA flow diagram of the literature selection process
3.2 Basic characteristics of the included studies30 studies [15,16,17,18, 26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51]included 3,637 TNBC patients who received anthracycline-free NAC regimens. Among these, 15 studies [15,16,17,18, 27, 29, 35, 36, 38, 41,42,43,44, 46, 50]were RCTs, 10 studies [28, 31, 33, 34, 37, 39, 45, 47,48,49]were cohort studies, and the remaining 5 studies [26, 30, 32, 40, 51]were other types of non-randomized controlled studies. The included taxane-based agents primarily consisted of docetaxel, paclitaxel, and nab-paclitaxel, while the platinum-based agents mainly were cisplatin, carboplatin, and lobaplatin. Only one RCT [15]explored and compared the effects of a taxane-plus-platinum NAC regimen versus a taxane-plus-platinum-plus-anthracycline regimen in TNBC patients. The baseline characteristics are detailed in Table 1 [15,16,17,18, 26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51].
Table 1 Basic characteristics of the included studies3.3 Quality assessment resultsFor RCTs, quality assessment was conducted following the guidelines of the RoB 2.0 tool. The included RCTs exhibited a certain level of risk, primarily in the selective reporting domain, as it was not possible to determine whether multiple analytical methods were employed in each study. The overall assessment results are presented in Supplementary Fig. 1, while detailed evaluations of the five domains are provided in Supplementary Fig. 2.
For cohort studies, quality was evaluated through the Newcastle-Ottawa Scale (NOS). The encompassed cohort studies did not receive scores for non-exposed cohort selection. Furthermore, regarding study comparability, given that all outcomes investigated in this study were rates, certain comparability criteria were deemed inapplicable. Except for the study by Riccardo Lobefaro et al. [47], no included studies received scores for comparability. Detailed assessment results are presented in Supplementary Table 1.
For non-randomized studies, MINORS was utilized for evaluation. Two studies were single-arm studies, while three studies included a control group. Among these, only one study [30]was classified as of moderate quality, whereas all others were considered of relatively high quality. Assessment results are detailed in Supplementary Table 2.
3.4 Meta-analysis results 3.4.1 Two-year OSTwo studies reported the two-year OS rate in patients with TNBC who received anthracycline-free NAC regimens. Given the limited number of studies, the preliminary pooled analysis estimated a two-year OS rate of 95.38% (95% CI: 86.64%-98.50%; I² = 0.00%, P_H = 0.65). Further details are displayed in Fig. 2(a).
3.4.2 Three-year OSFour studies reported the three-year OS rate in the TNBC population who received anthracycline-free NAC regimens. The preliminary pooled analysis estimated a three-year OS rate of 94.63% (95% CI: 87.91%-97.71%; I² = 62.00%, P_H = 0.05). Further details are illustrated in Fig. 2(b).
3.4.3 Five-year OSFive studies reported the five-year OS rate in patients with TNBC who underwent anthracycline-free NAC regimens. Our preliminary pooled analysis estimated a five-year OS rate of 86.97% (95% CI: 80.76%-91.39%; I² = 81.30%, P_H = 0.00). Further details are provided in Fig. 2(c).
A subgroup analysis stratified by the country of origin of the study population revealed that the pooled five-year OS rate was 91.00% (95% CI: 82.00%-95.00%; I² = 82.30%, P_H = 0.02) for studies conducted in China, 81.00% (95% CI: 74.00%-86.00%; I² = 44.10%, P_H = 0.18) for those conducted in Germany, and 85.00% (95% CI: 81.00%-88.00%) for a single study comprising populations from Spain and the United States. In the subgroup analysis, statistically significant differences in five-year OS rates did not exist among subgroups (P_intergroup = 0.12). Further details are provided in Supplementary Fig. 3.
A subgroup analysis based on specific chemotherapy regimens showed that two studies employing NAC with docetaxel plus carboplatin yielded a pooled five-year OS rate of 85.00% (95% CI: 82.00%-88.00%; I² = 0.00%, P_H = 0.48), while three studies utilizing paclitaxel plus carboplatin had a pooled five-year OS rate of 87.00% (95% CI: 77.00%-93.00%; I² = 90.20%, P_H = 0.00). The subgroup analysis revealed no statistically significant difference in five-year OS rates across chemotherapy regimens (P_intergroup = 0.75). Further details are provided in Supplementary Fig. 4.
3.4.4 OSNine studies reported the OS rates in individuals with TNBC who received an anthracycline-free NAC regimen. This study defined “OS rates” as the percentage of individuals were still alive among TNBC patients who received an anthracycline-free NAC regimen after the last update of the original study data.
The pooled analysis demonstrated a OS rate of 69.92% (95% CI: 41.65%-88.33%; I² = 97.20%, P_H < 0.01). Detailed information is presented in Fig. 2(d).
Sensitivity analysis indicated that the study by Ruo-Xi Wang affected the stability of our results. After this study was excluded, the pooled OS rate increased to 75.43% (95% CI: 47.97%-91.09%; I² = 96.00%, P_H < 0.01). Further details are provided in Supplementary
Comments (0)