
Remember me



This study presents a case of a 69-year-old male patient with a known history of prostate cancer. He had previously undergone radical prostatectomy and pelvic lymph node dissection. He has been on regular follow-up, during which recent imaging and biopsy confirmed the presence of metastatic SCC involving the peritoneum and omentum.
The patient is a non-smoker. His family history is notable for malignancy, with his son being diagnosed with early-onset colon cancer at age 37. The patient underwent a radical prostatectomy and pelvic lymph node dissection for prostatic acinar adenocarcinoma. The pathology report indicated a Gleason score of 7(4 + 3) and extracapsular extension. Postoperative prostate-specific antigen (PSA) levels was 0.1 ng/mL shortly after surgery and salvage external-beam radiotherapy to the prostate bed was delivered with a six-month course of androgen deprivation therapy.
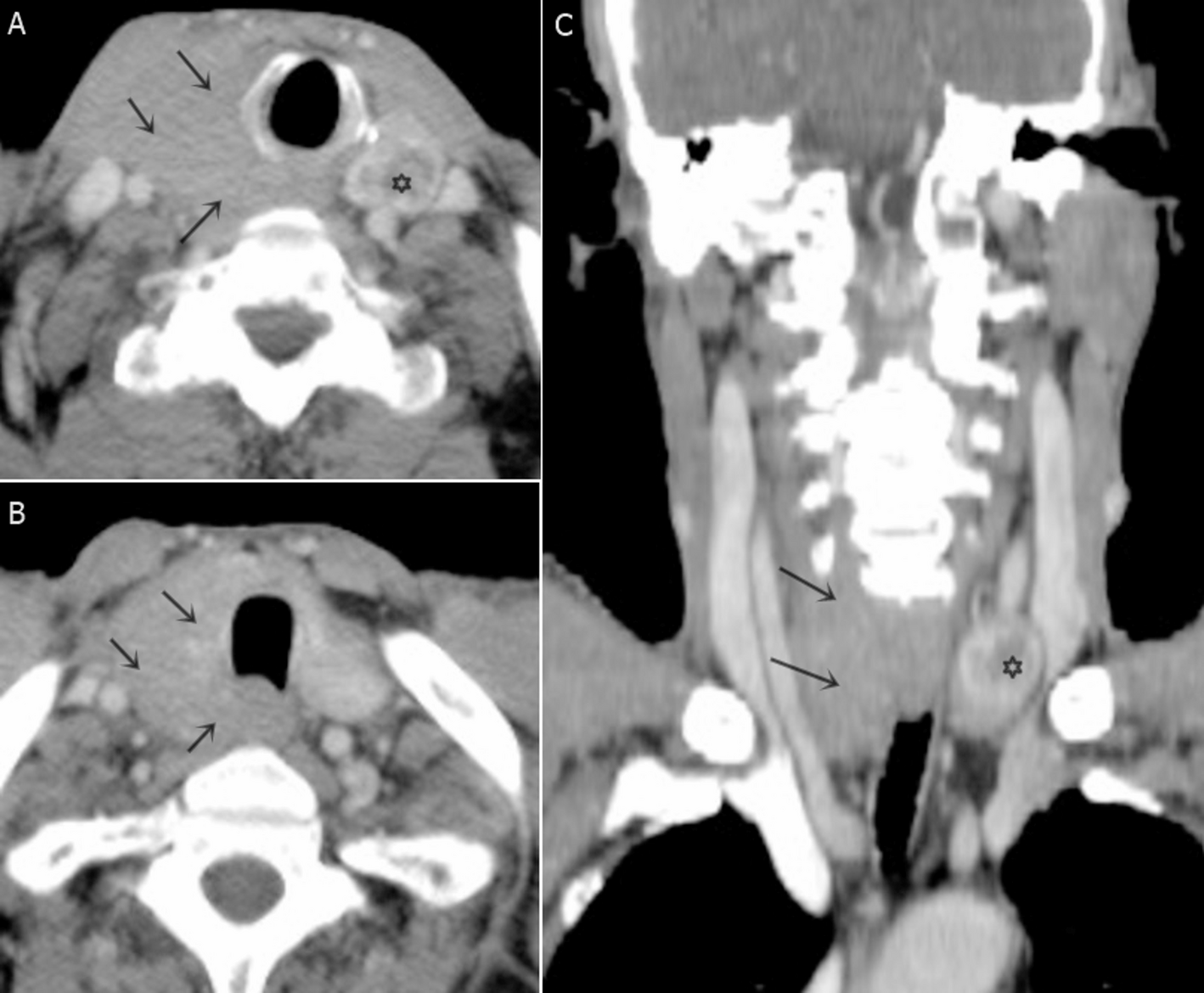
2.1 Presentation and DiagnosisTwo years after his initial treatment for prostate cancer, the patient complained of progressive abdominal distention and colicky abdominal pain that had been ongoing for three months before the current evaluation. On examination, vital signs were stable (BP 128/75 mmHg, HR 82 bpm, afebrile), the abdomen was tense with a positive fluid wave, and the rest of the systemic examination was unremarkable. Upon further investigation, a CT scan revealed moderate ascites (increased abdominal fluid) and nodular thickening of the peritoneum, indicating the presence of metastasis. His serum PSA level at presentation was 4.4 ng/mL. Additionally, there was an increased omental thickening, with a maximum thickness of 1.6 cm (Fig. 1).
Fig. 1
Staging CT (17 October 2020) shows large volume ascites (a), extensive peritoneal metastasis (arrow in b) and omental carcinomatosis (arrows in c)
To determine the primary origin of the metastatic carcinoma, an omental biopsy was performed. Histopathological examination of the biopsy confirmed SCC with immunohistochemical staining positive for markers such as Synaptophysin, Chromogranin, TTF-1, and focal CDX2 (Figs. 2 and 3). However, the cells were negative for CK7, CK20, PSA, and GATA-3 (Figs. 4). Based on the immunoprofile, a primary lung origin was favored, while GI or pancreatic origin was considered less likely.
Fig. 2
Histology of the tumor shows round/oval blue cells with minimal cytoplasm, small to medium-sized, and necrosis and apoptosis of individual cells
Fig. 3
Histology of the tumor showing wide peritoneal infiltration by small cell carcinoma
Fig. 4
Histology showed tumor cells staining positive for synaptophysin and TTF-1
Given the absence of a clear primary site, a broad differential diagnosis, including primary lung, GI, and pancreatic origins, was considered before reaching a conclusion. The diagnostic work-up was coordinated with input from oncology, pathology, and radiology teams.
PET/CT (Supplementary Fig. 1 A) demonstrated diffuse hypermetabolic omental and nodular peritoneal thickening associated with abdominopelvic ascites. These findings were consistent with biopsy-proven occult primary or primary peritoneal SCC. Minimal bilateral pleural effusion was observed, without definitive hypermetabolic lesions in the pancreas, GI system, or elsewhere. Esophagogastroduodenoscopy and colonoscopy revealed no tumor growth. Considering the diagnosis of SCC of an occult primary origin, palliative chemotherapy with carboplatin/etoposide is recommended.
2.2 Treatment and response and surgical consultationThe patient began chemotherapy with carboplatin/etoposide. Following significant GI toxicity and febrile neutropenia after the first chemotherapy cycle, subsequent doses were appropriately reduced, which improved tolerability. Supportive care, including antiemetics, growth factors for neutropenia, and nutritional support, was provided to mitigate chemotherapy-related side effects.
After 2–4 cycles, follow-up CT demonstrated marked reduction in nodular omental thickening and resolution of ascites, consistent with partial response to treatment. By the 6th cycle of chemotherapy, imaging showed no definitive metastatic omental deposits, no ascites, enlarged retroperitoneal lymph nodes, or lung metastases (Fig. 5). The patient’s symptoms, including abdominal cramps and fullness, significantly improved.
Fig. 5
Restaging CT shows remarkable response to treatment; characterized by absence of ascites, minimal remaining omental (arrow in a) and peritoneal (arrow in b) thickening
Since there was no evidence of disease outside of the omentum/peritoneum, the possibility of primary peritoneal SCC increased. The GI multidisciplinary team discussed the case for possible Cytoreductive Surgery + Hyperthermic Intraperitoneal Chemotherapy (CRS + HIPEC). After reviewing the available research and consulting specialized centers overseas, the patient was offered HIPEC as a potential treatment for his condition. However, he refused the treatment due to potential risks and limited evidence supporting its benefits. Follow-up CT initially showed no disease recurrence; however, a subsequent scan revealed progression in the size of a few peritoneal deposits. (Fig. 6).
Fig. 6
Restaging CT shows recurrence of peritoneal deposits in several locations. The most pronounced lesions are in the subhepatic fat (arrow in a), in the prevescical area (arrow in b) and I the left upper quadrent (arrow in c)
The same chemotherapy regimen was restarted. The patient responded positively after six cycles. Chemotherapy was stopped as he showed a complete response with no measurable disease. However, six months later, CT showed disease progression with new omental and peritoneal lesions but no metastasis elsewhere. Given his high sensitivity to the carboplatin/etoposide regimen and good tolerance, the same chemotherapy was pursued again. He completed six cycles and follow-up CT scans showed excellent response, including complete resolution of metastatic deposits and ascites, with no new metastasis. Details of the treatment cycles are summarized in Supplementary Table 1.
2.3 Current condition and patient educationThe patient consistently demonstrated a thorough understanding of his condition and treatment options and actively participated in shared decision-making. He was informed about the disease course, potential risks and benefits of therapies, and the importance of regular follow-up. Psychosocial support was also provided to address the emotional and logistical challenges associated with his diagnosis and treatment.
As of March 2025, the patient remained clinically stable (ECOG PS = 1) with no abdominal pain, nausea, or vomiting, and reported good appetite and stable weight. Laboratory values were unremarkable (hemoglobin level, 13 g/dL, creatinine 0.9 mg/dL). Follow-up imaging revealed no evidence of recurrent peritoneal or distant metastasis (Fig. 7).
Fig. 7
Restaging CT shows minimal peritoneal thickening in the subhepatic fat (arrow in a), appendiceal surface (arrow in b), and perivescical area (arrow in c)
Comments (0)