Among HIV-infected individuals, thyroid dysfunction is a common complication, but there is a notable gap in understanding the effects of HIV treatment on thyroid function, particularly in patients whose HIV is well-managed and suppressed. In this study, the overall prevalence of thyroid dysfunction in PLWH was 51.9% compared to 3.1% in HIV-negative healthy controls. These findings are consistent with other studies that indicate an increased incidence of thyroid disease among HIV-positive individuals compared to the general population [10, 25, 26]. The most common types of thyroid dysfunction identified among participants were subclinical hypothyroidism (44.1%), hypothyroidism (5.6%) and subclinical hyperthyroidism (1.3%), consistent with other previous findings [18, 27, 28]. These results indicate that patients with HIV can develop a variety of thyroid hormone abnormalities, with subclinical hypothyroidism being the most common thyroid abnormality among HIV-positive individuals.
However, some studies [10, 26] have reported clinical hypothyroidism as the common thyroid dysfunction in HIV-infected participants. The differences in the conclusions of these studies could be variations in the criteria for defining clinical hypothyroidism and subclinical hypothyroidism and differences in disease progression. Hypothyroidism in HIV has been associated with opportunistic infections that hinder thyroid function [29] since thyroid gland failure can result from the infiltration and destruction of the gland by opportunistic infections that often persist in PLWH [30]. Overall, our findings suggest that thyroid disorder is common among PLWH with increased prevalence of subclinical hypothyroidism hence a need for regular screening for thyroid disorder in PLWH.
Abnormal thyroid function has been associated with the virus independent of other factors [25], but there is some indication that an increasing number of patients on HAART are presenting with thyroid issues [10]. Therefore, it remains uncertain whether thyroid dysfunction in HIV patients is due to the virus, complications from the infection, HAART, disease progression, or other contributing factors. We analyzed the association of thyroid dysfunction in HIV-infected participants and several variables including age, HAART regimen and exposure, duration of HIV infection, coinfection and CD4 count. We found a positive correlation between HIV, HAART regimen and exposure, viral suppression status, duration of HIV infection, age, and co-infection with thyroid dysfunction. There was a higher prevalence of thyroid dysfunction in HAART-exposed HIV non-suppressed participants than in HAART-exposed HIV-suppressed patients, suggesting the role of the virus in thyroid abnormalities. Durable viral suppression improves immune function and overall quality of life [31] hence low risk of HIV co-morbidities.
On the contrary, viral non-suppression can result in an increased risk of general body dysfunction among them thyroid dysfunction as shown in the present study. Another factor that was positively associated with thyroid dysfunction in this study was the duration of HIV infection with the median duration of infection. As duration on ART among people living with HIV increases there was a significantly high chance, they will develop thyroid dysfunction (r = 0.49, p < 0.001). This is similar to another study [10] that found participants with longer HIV duration having lower FT3 and FT4 levels, indicating a higher possibility of hypothyroidism.
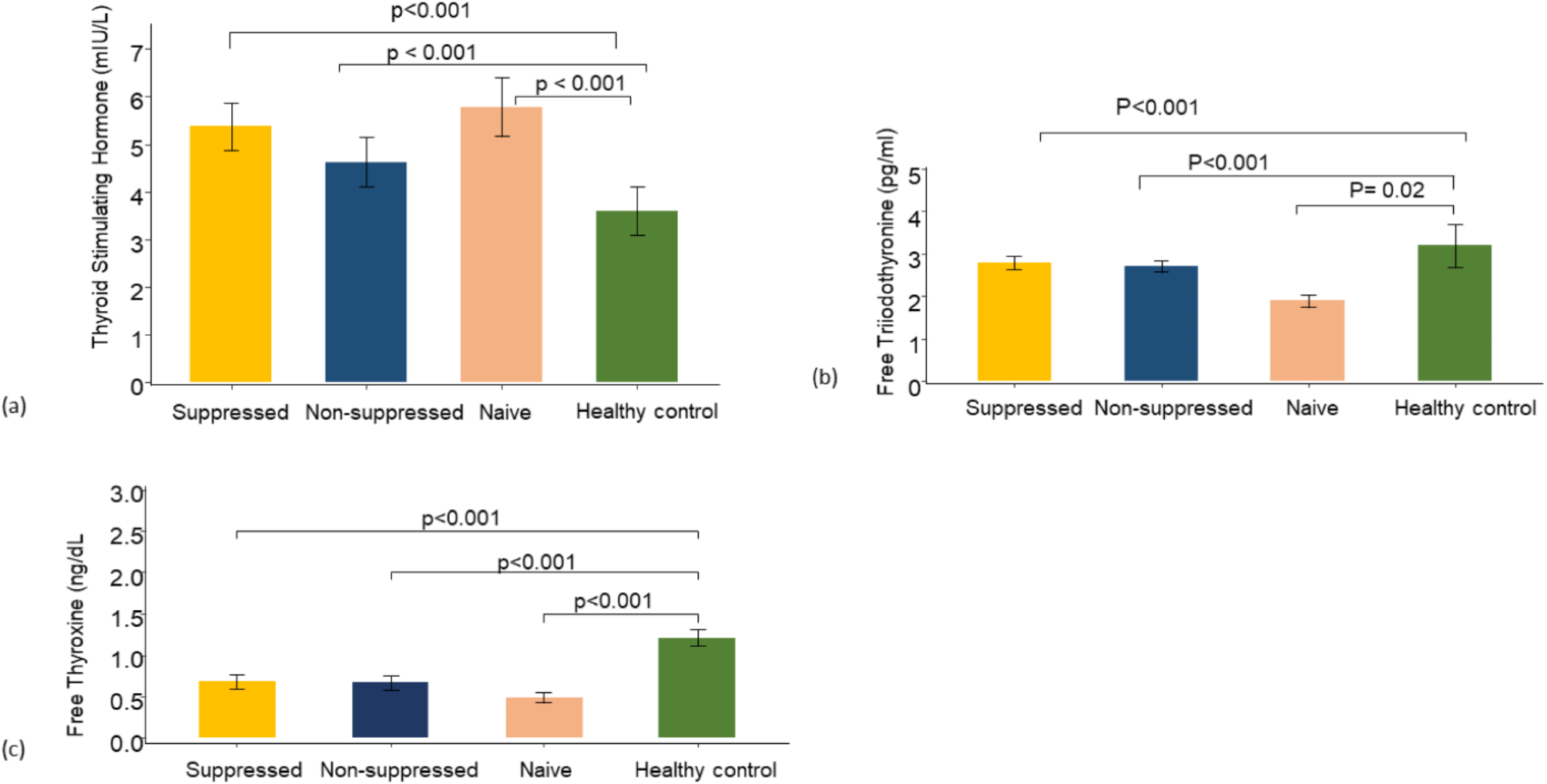
In Kenya, HAART is started on all PLWH, regardless of WHO clinical stage or CD4 cell count, per the national standards for HIV testing and treatment. In this study, the duration of HIV infection and HAART treatment duration was similar in the group receiving HAART hence separating the duration of HIV infection from the duration of HAART was not possible to conclusively attribute either to the increased risk of thyroid dysfunction. However, the positive correlation between HAART exposure and thyroid dysfunction in PLWH was shown by the higher occurrence of thyroid dysfunction in the group receiving HAART than in the HAART-naïve group. FT3 and FT4 levels were significantly higher in the HAART-exposed group compared to HAART naïve groups with no significant difference in the serum level of TSH. This indicates a possibility that HAART has a role in the development of thyroid abnormalities in PLWH.
Since the start of HAART treatment in Kenya, the regimens have been revised from time to time in concurrence with the WHO guidelines. Accordingly, DTG, an effective, tolerable anchor treatment [32] combined with two other INSTI is the preferred regimen, with the majority of participants in the HAART group on this regimen. There was a significant difference no notable variation in FT3 and FT4 thyroid hormone levels between the INSTI and PI regimen treatment groups. However, TSH levels were above normal ranges and significantly higher in the PI backbone HAART regimen compared to the INSTI backbone regimen. Stavudine has been linked to lower FT4 levels and hypothyroidism [26, 28, 33] whereas the role of other regimens, such as integrase inhibitors (INI) and PI, in impairing thyroid function has yet to be fully investigated [34]. However, the finding from this study suggests the role of PI in thyroid abnormalities. Dysregulation of pro-inflammatory cytokines during HAART [35] and/or a mitochondrial toxicity [36] as a result of the drugs may interfere with synthesis and metabolism of thyroid hormones hence a possible mechanism which HAART impact thyroid function.
Further, the risk of developing thyroid dysfunction was significant associated with TB-coinfected participants. In other studies, TB has also been associated with the development of thyroid abnormalities [37], especially with subclinical thyroid dysfunction in PLWH [38, 39]. Additionally, medications used to treat the opportunistic infections common in PLWH have been shown to affect the thyroid gland causing abnormality in hormone levels [25]. For instance, Rifampin used for TB treatment, a common infection in PWLH has been shown to diminish circulating thyroid hormone levels [40]. However, whether development of thyroid dysfunction is due to TB or TB medication or a combination of both remain unraveled.
Age and gender are crucial factors in the onset of thyroid dysfunction in PLWH [34]. This study did not find a difference in the prevalence of thyroid dysfunction between females and males. This is contrary to other studies [17, 34, 41] that have shown females are more at risk of developing thyroid dysfunction among PLWH. However, there was a higher risk of developing thyroid dysfunction with an increase in age in this study, though the risk was not significant. This is similar to other studies [41, 42] that have reported an increased prevalence of thyroid dysfunction in older PLWH.
HAART treatment may lead immune recovery, as evidenced by increased CD4 lymphocyte counts, a lower risk of opportunistic infections, and improved life expectancy. In this study, there was an inverse correlation between CD4 count and thyroid dysfunction. indicating a trend that as CD4 counts improve, the risk of thyroid dysfunction reduces. This is consistent with a study [43] that found subclinical thyroid dysfunction was correlated to declining CD4 counts. Overall, these findings suggest a link between thyroid dysfunction and HIV disease progression.
Though the study found a positive correlation between HIV, HAART, duration of HIV infection, age, and TB with thyroid dysfunction, only HIV, duration of HIV infection, and TB infections were the factors significantly associated with thyroid dysfunction. The results of this should be interpreted with the limitations of the study in mind; first, the sample size was small and sampled form a single hospital, which may preclude the generalizability of the findings. Second, certain factors like iodine in diet which have implications on thyroid function were not considered. Third, this was a cross-sectional study without follow-up to identify changes in thyroid function. A prospective study with a longer follow-up could add data related to the effect of diet intake on thyroid dysfunction in HIV patients.

Comments (0)