Branchial cysts are the most common pathological diagnosis of cystic masses in the lateral neck region, accounting for 58.6–80.3%. Among malignant lesions, the most common is squamous cell carcinoma, whereas differentiated thyroid carcinoma is very rare, accounts for only 0.8–1.5% of cases. The differential diagnosis of a cystic mass in the lateral neck from the literature [14,15,16,17] and the present case are listed in Table 1. Cystic metastatic papillary thyroid carcinoma without a histologically identifiable primary tumor within the thyroid gland is very rare. This category was introduced by the literature in which a thyroid gland lesion is determined to be benign or normal by pathologic and imaging examinations, but thyroid carcinoma metastases are found in either local lymph nodes or distal organs [11, 18, 19]. This category is often extremely difficult to distinguish from laterocervical lymph node metastasis from primary neoplastic involvement of ectopic thyroid cancer [12, 20].
Table 1 Differential diagnosis of cystic masses of the lateral neck from the literature and the present caseIn the present case, several factors might explain the diagnosis of lymph node metastasis from PTC. First, the right node metastases could not represent any normal thyroid follicular tissue. Second, the right mass showed a local papillary tumor surrounded by lymphocytes with germinal centers, which indicated no evidence of ectopic thyroid tissue. Third, a meticulous and exhaustive pathologic examination was performed on our patient, but it failed to reveal any lesions in the total thyroid. Some studies have reported that undetected primary thyroid carcinoma is likely to be overdiagnosed, as histopathological examination may miss a microcarcinoma < 3 mm in size that has the potential to develop metastases [21, 22]. In this case, the histologic sections had a mean thickness of 3 mm, which provided a good possibility for the detection of even smaller lesions (< 3 mm). Finally, an ectopic site of origin of thyroid cancer, including the struma ovarii and other sites (lingual, sublingual, thyroglossal, laryngotracheal), was not present on post-therapeutic whole-body scintigraphy. Postoperative low levels of serum thyroglobulin and antithyroglobulin antibodies also excluded the patient from an ectopic PTC diagnosis.
Another possible hypothesis is that the tumor spontaneously regresses or that some immunologic or host-resistance factors prevent the growth of the carcinoma and eventually cause obliteration [23,24,25]. The present case may be explained by this rare phenomenon of metastatic disease without an identifiable primary tumor within the thyroid. In PTC, fibrosis with Hashimoto’s thyroiditis may be an important symptom of partial or total tumor regression. In a case of bone metastasis from PTC, no malignant lesion was discovered in thyroid with diffuse thick fibrosis and lymphocytic infiltration [19]. In another case of right upper neck lymph metastasis from PTC, no primary tumor was found in the thyroid; however, hyalinized imaging of the thyroid indicated that a micropapillary thyroid carcinoma might have spontaneously disappeared [26]. In the present case, the mechanism of tumor regression remains unknown, as there was no evidence of Hashimoto’s thyroiditis or signs of neoplastic cell phagocytosis by macrophages. Host resistance mechanisms may cause PTC in the thyroid to fade away following cervical lymph node metastasis.
Despite the extreme rarity of these cases, there are no standard evidence-based recommendations regarding optimal treatment. Cystic metastasis from occult PTC may be a very indolent lesion and therefore mimic the clinical course of benign lesions [27]. It may arise primarily from the thyroid, which undergoes cystic degeneration in the context of cervical lymph node metastasis [28]. The most reasonable treatment approach is based predominantly on imaging studies of the orthotopic thyroid gland and cervical lymph nodes that could guide the extent of the surgery. Treatment with radioiodine after orthotopic thyroidectomy should be based on individualized risk stratification according to the guidelines [29]. Regular follow-up is required to monitor the possibility of recurrence or distant metastasis. In this case, although no evidence of primary tumor in thyroid gland was detected in preoperative imaging. We classified the patient as a high risk for recurrence or metastasis due to a metastatic lymph node > 3 cm according to the American Thyroid Association (ATA) guidelines [29]. The total thyroidectomy was performed to avoid missing thyroid microcarcinoma and to make preparation for possible I-131 ablation after multidisciplinary consultation. The stimulated Tg didn’t reach the category of excellent response, considering the high risk of recurrence or metastasis, I-131 treatment was performed. Previous research [30] reported a patient with an isolated metastatic lymph node (3 cm×2 cm). Routine excision of metastatic lymph node and a subtotal thyroidectomy was subsequently performed, but without I-131, and the patient had no signs of recurrent disease two years later. It has been suggested that in patients with isolated lymph node metastases, particularly those lymph nodes less than 3 cm, a more conservative approach could be considered.
Studies [9, 10, 13, 19, 27] have shown that these cystic masses, which are pathologically confirmed as metastatic PTC, often have several characteristics, such as the following: they usually occur in patients older than 30 years, are larger than 2 cm, there is no significant sex difference in the incidence (Table 2). Pathological examination after resection is an important method to confirm the diagnosis. Although these patients have no signs of primary thyroid tumor on preoperative ultrasound, papillary microcarcinoma (PMC) might be found via postoperative pathology in some patients. When we encounter cystic masses of the lateral neck in patients older than 30 years, the possibility of lymphatic metastasis of papillary thyroid carcinoma should be considered, although this probability is relatively low.
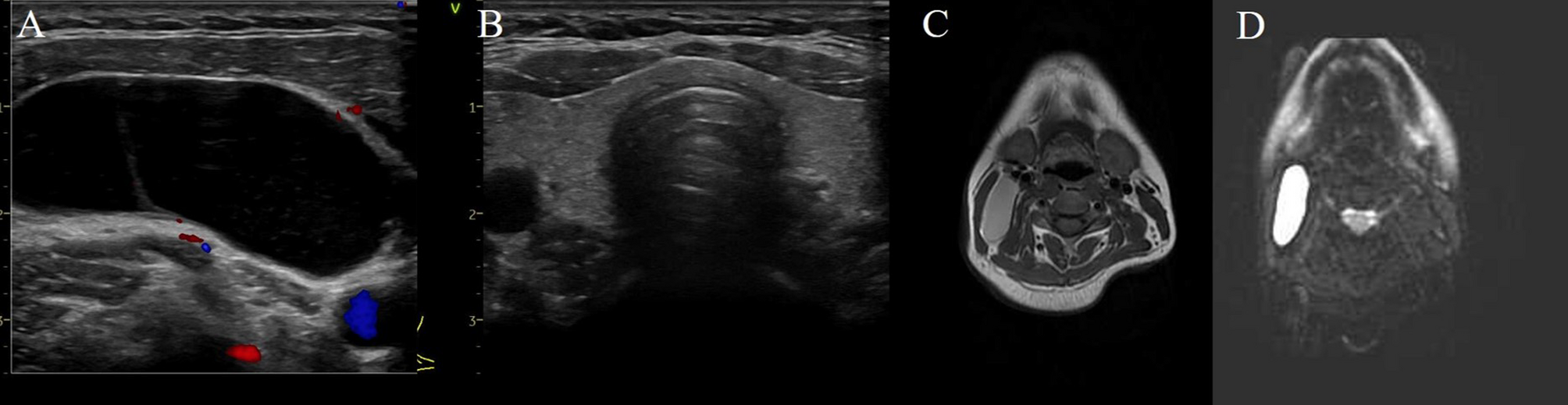
Table 2 Reported cases of metastatic PTC presenting as a cystic mass of the lateral neck without a detectable primary tumor on preoperative ultrasonography from the literature and the present caseFine-needle aspiration biopsy (FNAB) is useful for the diagnosis of suspected neck masses, especially solid masses. However, it is often limited in cystic lesions with a paucity of cellular material to target, resulting in poor diagnostic accuracy. In this case, the cystic mass was filled with fluid, it was difficult to obtain solid tumor components by FNAB. In addition, the probability of isolated lymph node metastasis without a primary tumor is extremely low, so cytological puncture was not performed. The fine-needle aspiration (FNA) of the cyst with thyroglobulin FNA (TG-FNA) washout may help to confirm the diagnosis and improve clinical decision-making, with the sensitivity of detection of the metastatic lymph node to 97.5%, even with negative cytology of FNAB [31]. However, because it is so rare, it is not considered first in clinical practice.
In conclusion, we report a rare case of a lymph node metastases of papillary thyroid carcinoma as a giant cervical cyst, wherein neither ultrasonography nor careful pathological examination detected PTC in the thyroid gland. Meticulous pathological evaluation of surgical specimens is key to making a definitive diagnosis. The prognosis is usually favorable.

Comments (0)