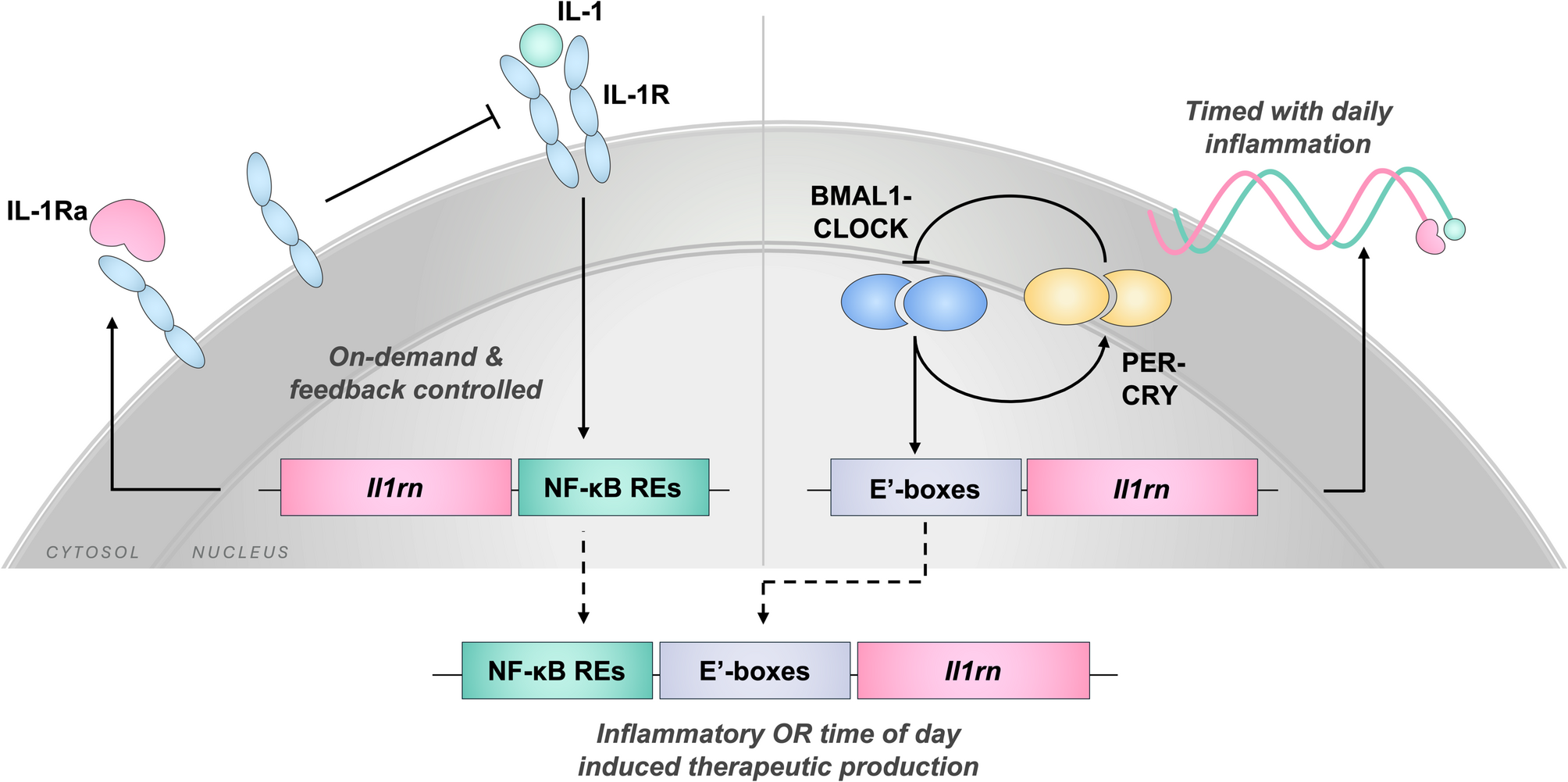
In this study, we designed and tested a novel synthetic gene circuit responsive to both circadian and inflammatory signaling pathways for timed chronogenetic and inflammatory feedback-controlled cell-based drug delivery. This gene circuit successfully demonstrated both independent and dual-responsive synthesis of biologic drugs on demand. In the absence of an inflammatory challenge, this circuit responded to endogenous circadian transcriptional feedback signals through E’-box elements, resulting in autonomous cycling over a 24-hour period. During inflammatory challenge, this circuit had enhanced output that was regulated through a central inflammatory pathway, allowing the circuit to sense and respond to its dynamic environment. With this OR-gate digital logic, either inflammatory or time-of-day input resulted in disease-relevant activation for fine-tuned therapeutic release. Through this dual response, the circuit demonstrated a proof-of-concept design to address the complexity of flares in RA, JIA, or other inflammatory diseases that occur on both daily and long-term scales.
Physiologically, the concentration of IL-1β in synovial fluid and serum of RA patients is approximately 0.1 ng/mL, although this can vary patient to patient [30, 31]. Similarly, 1 ng/mL IL-1β has been shown to affect circadian rhythms [32]. Therefore, we assessed the dose-response for circuit activity in monolayer cells at 0, 0.1, or 1 ng/mL IL-1β and chose to assess outcomes in iPSC-derived pellets at the maximum dose of 1 ng/mL to ensure effectiveness at levels greater than the expected physiologic condition. As shown by both bioluminescent reporters for real-time circuit activation kinetics and the therapeutic release profile of IL-1Ra at discrete timepoints, the NFκB.E’box promoter had significantly higher activation in the presence of an inflammatory challenge than in its absence. While cumulative IL-1Ra measured from the culture media at specific timepoints cannot show a cyclical change in output, we have demonstrated that, at a basal level, the rate of change in IL-1Ra therapeutic production from E’box-IL1Ra is cyclical with an approximately 24-hour period [22]. Without NF-κB responsiveness, we have previously shown that there was no significant change in chronogenetic IL-1Ra release during IL-1β challenge [22]. In the dual-responsive circuit developed in this study, there is enhanced output of IL-1Ra during IL-1β challenge in comparison to non-challenged controls, which can better address the short-term and long-term changes in inflammatory arthritis. This aligns with the output profile observed for NFκB-IL1Ra, which has shown a dose-dependent increase in IL-1Ra release with respect to IL-1 challenge that reached significance over unchallenged controls by 24-hours post-challange [2]. Additionally, previous reports have demonstrated that therapeutic IL-1Ra, produced by either NFκB-IL1Ra or E’box-IL1Ra gene circuits, protected circadian rhythms, suggesting that the dual-responsive circuit can maintain activity under pathological conditions, such as IL-1 challenge [22, 32]. Of note, on-demand inflammatory response that reaches significance between challenged and unchallenged conditions at 24-hours post-challenge may not generate a rapid enough response for dynamic inflammation in vivo. Other strategies to increase output rate could investigate the number and specific response elements driving inflammatory response or pursue transcriptional and translational efficiency optimization. However, supporting the utility of this design, our in vitro model of arthritis was protected in both the level of inflammatory activation measured by bioluminescence reporters and the tissue-level matrix and gene expression in comparison to control samples.
Traditionally, therapeutic drugs are delivered at prescribed times, such as daily or weekly, without regard to the dynamic disease state, effectively functioning as open-loop systems [33]. This approach contributes to a mismatch between the given and required dosage, which can lead to side effects while leaving the disease uncontrolled. In autoimmune conditions like RA and JIA, disease management can be exceptionally challenging, due to unpredictable flare ups in disease severity and medication responsiveness that can decrease over time [12, 34, 35, 36, 37]. With these challenges, closed-loop systems that use real-time input to provide therapeutic delivery when it is most beneficial may support improved disease control. Since cells have the necessary machinery to sense their environment and respond rapidly, adapting these tools to form gene circuits is a relatively straightforward extension of natural homeostatic mechanisms. Moreover, this contrasts constitutive delivery of therapeutics like IL-1Ra, which may even worsen arthritic outcomes, by delivering drugs according to both chronotherapeutic and on-demand strategies tailored to match disease dynamics [38].
The goal of this study was to generate a system that provided dynamic control of biologic drug synthesis across multiple time scales that are characteristic of inflammation in various autoimmune conditions such as RA and JIA. With this design, the gene circuit can be introduced with a single promoter-output cassette. While existing iterations of gene circuits target distinct environmental cues, including inflammatory, circadian, or mechanical activation alone, the dual-responsive circuit addresses two interconnected disease-relevant conditions, achieving more tunable control [1, 2, 3]. Others have successfully developed circuit systems in mammalian cells that include tools like amplification, feedback control, and digital logic for precise therapeutic delivery [5, 6, 39]. These elements support more controlled delivery; however, to achieve this level of regulation, orthogonal components are often required, which increases system complexity. Herein, we developed a system that does not require the introduction of non-native signaling molecules or transcriptional machinery for circuit transduction. Instead, we demonstrated increased circuit control through a dual-responsive promoter that activates through endogenous signaling pathways, creating a simple but multifaceted system.
In summary, this dual-responsive synthetic gene circuit has the potential to address challenges in synthetic gene circuit control for inflammatory arthritis. Beyond arthritis, other inflammatory diseases are implicated to have associated inflammatory and circadian changes, including but not limited to inflammatory bowel diseases and chronic airway diseases [40, 41, 42]. This proof-of-concept circuit design can be tailored to address a multitude of conditions. Herein, we demonstrated that E’-box-driven rhythms can be utilized in a dual-responsive system, but other phases in the 24-hour period can be targeted with circadian response elements like D-boxes or RREs [22]. Moreover, combinations of these elements may be able to encode circadian expression at even more precise times [43, 44]. Likewise, therapeutic output can be modulated based on the desired therapeutic protein, such as in previous efforts to generate circuits producing either IL-1Ra or soluble tumor necrosis factor receptor [4]. Since this system was developed in a cartilage model, the design can be translated to in vivo studies, as cartilage is avascular and aneural, and can be implanted subcutaneously for long-term therapeutic delivery [23, 45]. Previously, we have shown that bioengineered cartilage constructs edited to contain gene circuits can act as living drug delivery devices that sense and respond to environment cues. Using this translational strategy, proof-of-concept inflammatory and circadian-driven therapeutic delivery has been achieved in vivo [3, 23, 45]. With inflammatory responsive gene circuits, arthritis was mitigated in the K/BxN serum transfer model. Furthermore, efficacy of this strategy has been demonstrated up to 28-weeks post-implantation, suggesting long-term utility; however, further investigation on immunogenicity would be required prior to clinical application [45]. To dampen inflammatory activation, approximately 10- to 100-fold excess of IL-1Ra over IL-1 is necessary [46, 47, 48]. In vitro, we achieved approximately 100-fold excess of IL-1Ra over the IL-1 challenge within 24-hours, suggesting that this design can adequately produce a therapeutic dose. However, dosage can be modified by the geometry or number of cells per implant or the number of implants needed to optimize therapeutic efficacy. Therefore, this dual-responsive system serves as a prototype for future designs tailorable to specific disease scenarios.




Comments (0)