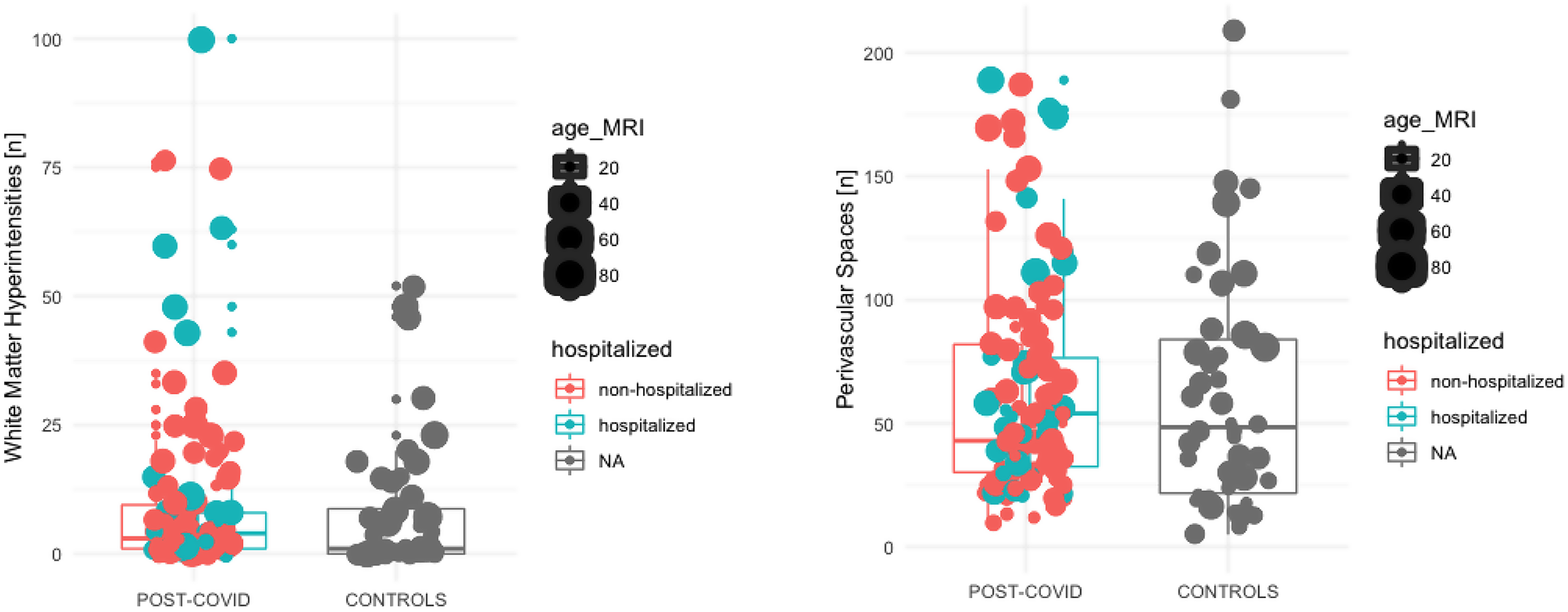
While numerous MRI features have been reported in subjects after severe COVID-19, or atrophy pattern on T1-weighted images, the frequency of neuroradiological findings in mild-to-moderate COVID-19 is unknown. Our findings underscore the importance of addressing the real-world clinical scenarios in which individuals with mild-to-moderate COVID-19 are referred for brain MRI due to non-focal, non-emergency neurological symptoms such as persistent headaches, subjective cognitive difficulties, or prolonged anosmia. These symptoms, while not emergent, are clinically relevant and reflect the ongoing need for further investigation in post-COVID care. In the present study, in 112 subjects who were prospectively imaged after mild-to-moderate COVID-19, no evidence of brain involvement using structural and advanced MRI at 3T was found. While the absence of evidence is no evidence of absence, our findings indicate that, in mild-to-moderate COVID-19, after around 228 days (sd: 140), there is no morphological evidence to suggest CNS involvement in a sample size of 112. This observation has the following implications. First, our findings are reassuring that structural brain involvement, which could remain subclinical, was not missed on a large scale in mild-to-moderate COVID-19, while COVID-19 -related involvement, also in the mildest COVID-19 cases, is clinically suggested by ageusia and anosmia [23]. Similar to previous literature, we did not find evidence of gross morphological brainstem involvement, which could be hypothesized in the course of cranial nerve-related CNS entry via cranial nerve V/I [24, 25]. Second, in the approximately 115 publications on CNS involvement demonstrated on brain MRI in subjects with severe COVID-19, a broad spectrum of CNS pathology has emerged, including vascular/ischemic lesions, (micro-)hemorrhages, cytotoxic lesions of the corpus callosum, and posterior reversible encephalopathy [2, 13]. To some extent, these features might also be seen in critically ill individuals without COVID-19, and, to this end, our findings do not indicate a COVID-19-related pathology in mild-to-moderate COVID-19. However, the reported imaging findings in cases with severe COVID-19 are, by far, not fully explained by critical illness alone, and endothelial dysregulation, as well as irregularities in coagulation, have been identified as components of COVID-19-related brain involvement [26, 27]. The absence of CNS involvement in our cohort is in line with a retrospective study that showed a correlation between lung and brain involvement in hospitalized COVID-19 patients with acute neurologic manifestations [28]. Third, perivascular inflammation has repeatedly been shown in autopsy cases of COVID-19, and enlargement of the perivascular spaces occurs in the course of acute inflammation in other CNS conditions [13, 29]. However, we did not find evidence of higher perivascular space counts in our cohort, suggesting that perivascular inflammation in mild-to-moderate COVID-19 is either below the detection level of our analysis, or absent at the time of acquisition (at a mean of 228 days after a positive PCR). Our volumetric analysis reproduced known influence of age and sex on grey matter volume, but we did not detected effect of post-COVID status. Furthermore a sub-analysis within the post-COVID group showed no significant impact of hospitalization status on grey matter volume.”
While cognitive decline is now increasingly recognized as a sequale of COVID-19, the literature is largely focused on structural brain findings, with little to no data on structed clinical neuro-radiological assessment of extensive MRI protocols [30].
This study has several limitations. As the cohort was prospectively recruited, there is a wide age range and gender was homogeneously distributed, but the sample size is limited. Considering the previously reported frequencies of neuroradiological involvement, e.g., (micro-)hemorrhages in 6.9% (95% confidence interval, 4.9-8.9%), in a recent meta-analysis, it should, however, have been sufficiently powered to detect cases, if this feature was present at a comparable frequency in mild-to-moderate COVID-19 [31].
In the present analysis, an assessment of COVID-19-related subjective clinical symptoms was performed with phone calls and a retrospective chart review and was available only in 50 individuals. While acceptable test criteria can be achieved with telephone assessments in domains comparable to those investigated in the present manuscript, our data do not provide a detailed clinical assessment of symptoms significantly affecting functional outcomes after COVID-19 [32]. Further, we likely have a lower power to detect clinical symptoms and we are limited to the assessment of symptoms known to be associated with the disease. While symptom data were collected from a subset of participants, this was not the primary focus of our study nor directly related to our outcome measures. We acknowledge this as a limitation but believe that the absence of complete symptom data does not diminish the relevance or value of our findings on structural brain changes in this population.
The vaccination program started in Austria in February 2021 for healthcare professionals and individuals at risk. In 48/112 subjects, brain MRI was acquired prior to February 2021. While vaccination status, including type of vaccination or the time post vaccination, are unknown, a sub analysis between those that received their MRI before and February 2021 did not show any group differences, data not shown.
While COVID-19 infections were excluded by medical chard review in the control cohort, we cannot exclude sub-clinical or non-reported infections in both, controls and the COVID-19 group.
We cannot provide detailed information on SARS-COV2 mutation status in our patients.
The mean follow-up interval in this cross-sectional study, from clinical symptoms to brain MRI, was 228 days, we cannot exclude structural brain MRI findings prior to or after this time point, but if present they would have been reversible from an imaging point of view, and findings after this interval will be determined with a follow-up study.
As the absence of prior neurological morbidity and thus brain MRI, was an inclusion criterion, it is impossible to assess the temporal course of the encountered imaging findings. So, while we did not observe cross-sectional group differences between controls and individuals after mild-to-moderate COVID-19 in white matter lesions and enlarged perivascular spaces and other structural brain MRI findings, we cannot exclude faster accrual rates over time.
The set of imaging sequences we selected for this analysis was chosen based on previous literature in the field [2, 31]. However, we might have missed cranial nerve involvement or leptomeningeal enhancement (described in the literature after the study was initiated), which would have required the acquisition of post-contrast T1-weighted images.
The limitations of this study also include a lack of stratification of the severity of the cases, beyond the information of whether they had been hospitalized.
Due to the limited clinical information, we did not include comorbidities (smoking, hypertension, diabetes) in our analysis.
Last, but not least, the McDonald 2017 criteria for dissemination in space were fulfilled in a 32-year-old female that was excluded from the analysis [33]. While SARS-CoV-2-induced demyelination has been suggested, we hypothesize that our case rather resembled an incidental finding of multiple sclerosis, as symptoms (consistent with a clinically isolated syndrome) were, upon inquiry, recalled in the year prior to the SARS-CoV-2 infection [34, 35].

Comments (0)