Advancing the diagnosis and management of pudendal nerve entrapment: The role of neurophysiological studies and imaging-guided infiltrations
Purpose
Pudendal nerve entrapment (PNE) diagnosis is not standardized. This leads to diagnosis delays, impacting quality of life and therapeutic outcomes. The main goal is to find the role of neurophysiological study (NFS) and Imaging-guided pudendal nerve infiltration (ImPNI) in PNE diagnosis and patient selection for surgery.
Methods
A retrospective, multicentric study was conducted. Patients with PNE refractory to conservative treatment were included. Patient data, including NFS results, ImPNI, and surgical outcomes, were evaluated. A visual analogue scale was used to assess intervention response. Test performance metrics for NFS and ImPNI and binary logistic regression were used to determine their predictive value for postoperative improvement.
Results
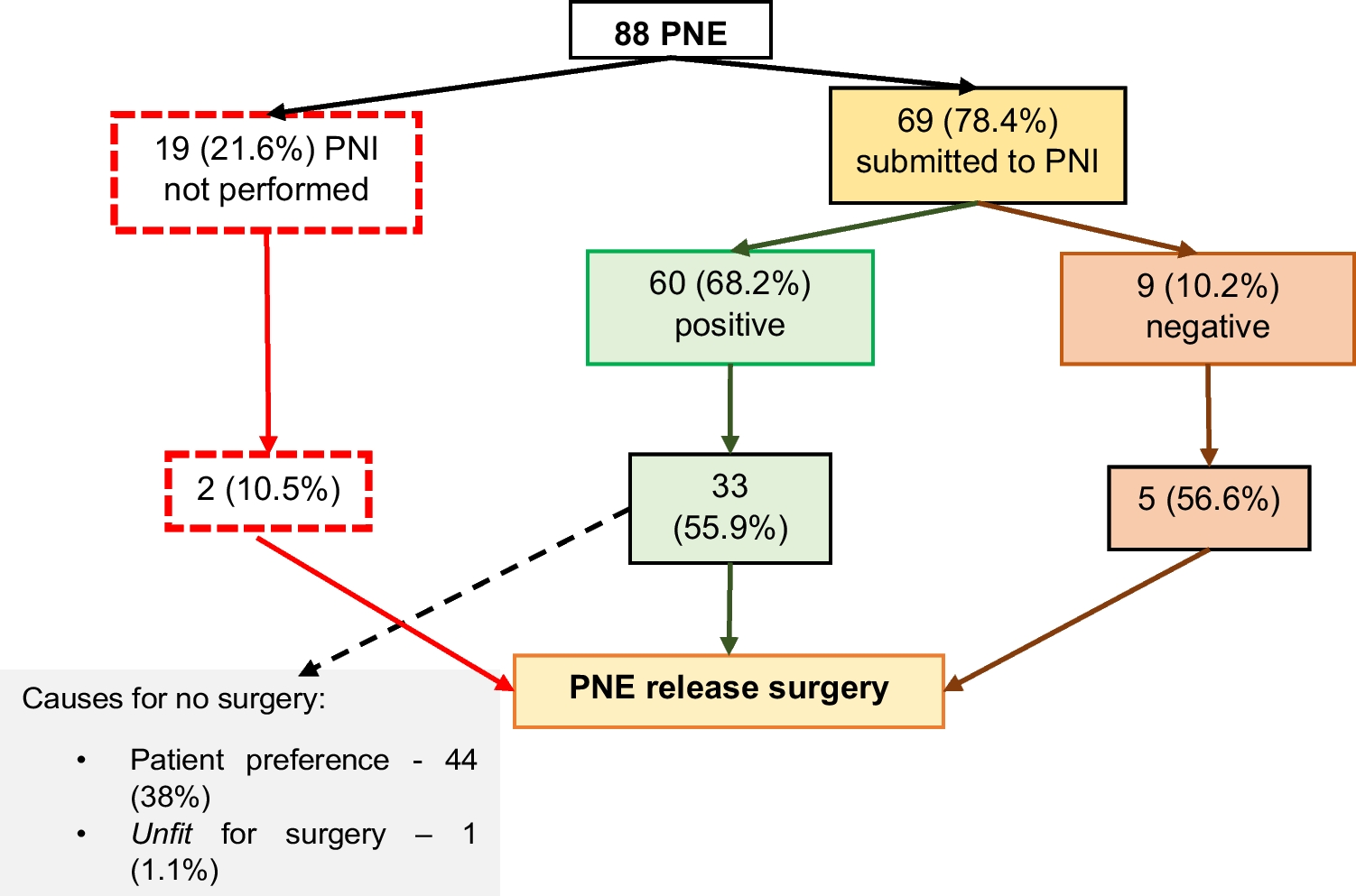
88 patients were diagnosed with PNE. All had NFS, and ImPNI was performed in 69 (78.4%), with 60 (68.2%) showing symptom improvement. Among the 40 patients (85%) who underwent pudendal nerve decompression surgery, 75% improved after surgery, and 20% did not.
The combination of NFS and ImPNI showed a sensitivity of 79% and a specificity of 85.7%, with a Positive Predictive Value (PPV) of 98% and a Negative Predictive Value (NPV) of 30%. NFS and ImPNI were significant predictors of surgical success with p-values of 0.013 [ 95% CI: -23.6—19.9] and 0.003 [95% CI: -20.6 -18.5], respectively. Primary limitations: retrospective design and the absence of a control group.
Conclusions
NFS and ImPNI are essential and highly reliable tools for diagnosing PNE. ImPNI is a valuable predictor of surgical outcomes. These findings enable precise patient selection for surgery, ensuring optimal surgical outcomes.

Comments (0)