This is the first study to conduct a quantitative assessment of the masticatory behaviors of patients with mandibular prognathism using a wearable device. The results showed that compared with participants with individual normal occlusion, patients with mandibular prognathism exhibited characteristic masticatory behaviors comprising a significantly smaller number of chews, significantly shorter mealtime, and leaning further forward while eating. The results also suggested that this masticatory behaviors in prognathic participants may be associated with maxillofacial morphology.
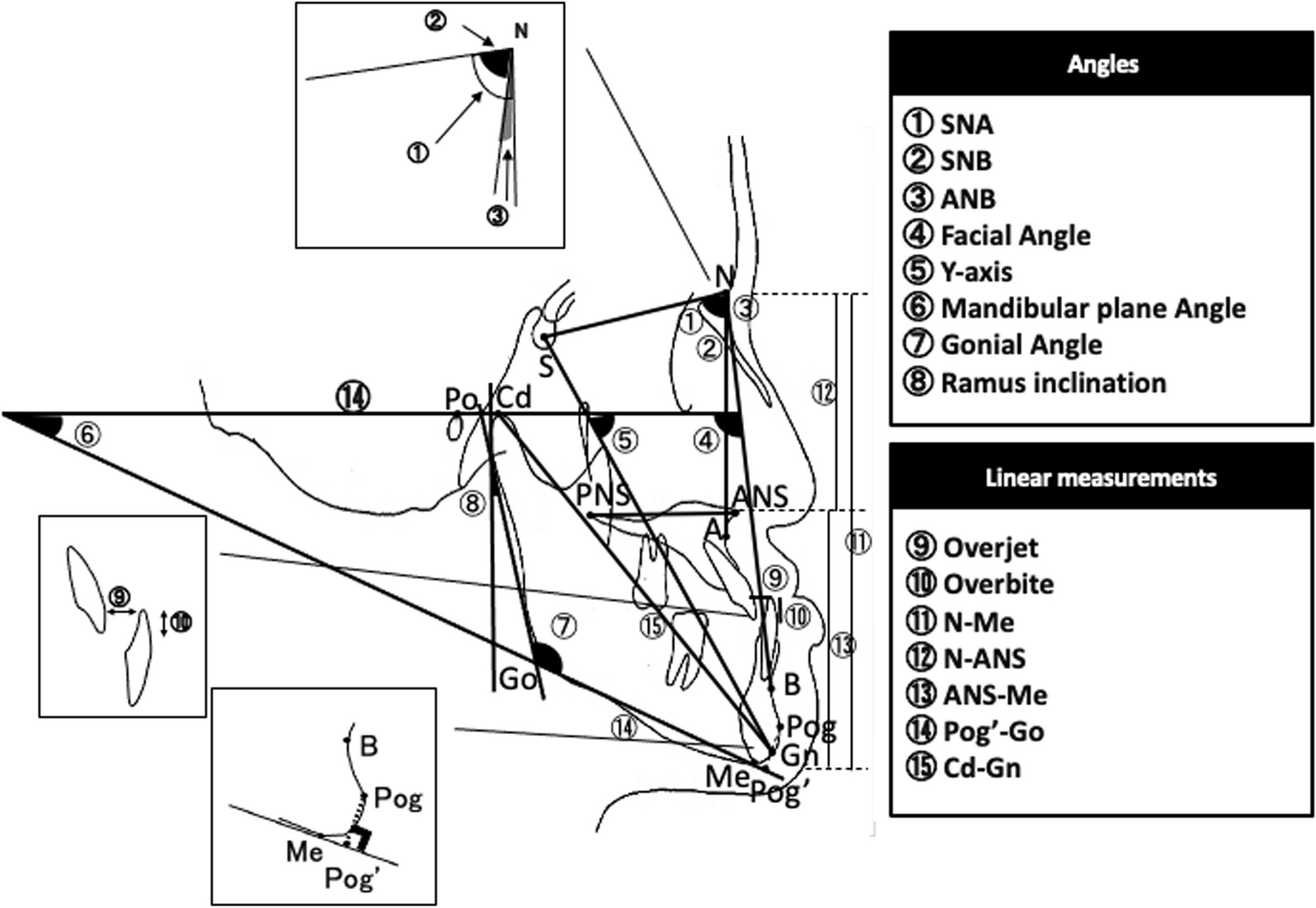
Mandibular prognathism is a misalignment of the positional relationship between the upper and lower dental arches causing a cross bite between the upper and lower front teeth. Either the maxilla is set too far back, the mandible is set too far forward, or both, meaning that the lower jaw projects anteriorly relative to the upper jaw, and, morphologically, this condition is characterized by a long mandible and a large gonial angle [11, 12]. The participants in the patient group in the present study exhibited the characteristic maxillofacial morphology of patients with mandibular prognathism, with mandibles that were located more anteriorly relative to the cranium than those in the control group, as well as a longer mandibular length and longer mandibular body length.
Among other indices, it has previously been reported that patients with mandibular prognathism have significantly lower masticatory performance, occlusal contact area, and maximum occlusal force than do participants with individual normal occlusion [13]. Patients with mandibular prognathism also find it harder than people with normal occlusion to eat a range of different foods in daily life [14], and participants with low masticatory performance reportedly swallow food as large particles [15], both of which may lead to a lower number of chews and shorter mealtime. The present results thus support those of previous studies, suggesting that patients with mandibular prognathism may not fully masticate food taken into the mouth but swallow it while it is still in large particles. However, there have been reports that the masticatory rhythm of patients with mandibular prognathism was unstable and prolonged [16], and that mastication time tended to be longer than that of participants with individual normal occlusion [13]. Those studies involved experimental systems in which the masticatory rhythm and time were measured when participants were instructed to chew for a specified number of times, rather than by monitoring masticatory behavior, and the different measurement method used is likely to have affected the results. Further studies that investigate parameters including masticatory performance are required in the future, as are comparative studies before and after surgery.
The device used in this study, the bitescan, has been investigated for accuracy in previous studies and is reported to be sufficiently reliable [7]. In addition, the bitescan is fitted with a three-dimensional accelerometer for postural evaluation, and it can measure both the movement and inclination of the head. The present measurements of head and neck posture while eating showed that the forward tilt angle was significantly lower in the patient group than in the control group, indicating that this group leaned forward while eating. Patients with mandibular prognathism reportedly tend to adopt a natural head position with the chin tucked in so that their mandibular prognathism is less obvious, out of a fear of being looked at [17]. In this study, even though bitescan calibration was conducted with the Frankfort horizontal plane parallel to the floor, the participants in the patient group may have been used to adopting a natural head position with their chin tucked in, and this may be why they leaned forward while chewing. One study using lateral cephalometric radiographs found that the resting tongue position of patients with mandibular prognathism was overall low and far from the palate, with the tip of the tongue tending to be on the lingual side of the lower front teeth [18]. The position of the hyoid bone has been reported to vary depending on head and neck posture [19], and patients with mandibular prognathism, who have morphological and functional discrepancies of the stomatognathic system, may change the position of the hyoid by leaning forward while chewing to encourage tongue elevation and make it easier to chew and swallow.
The present investigation of the associations between masticatory behavior and maxillofacial morphology found that in the control group, there were significant negative correlations between the number of chews per bite and Mp, Go, and N-Me. In contrast, in the patient group, the chewing rate was significantly negatively correlated with ANB and significantly positively correlated with Pog′-Go, whereas for the items related to posture, anteroposterior head and neck posture were significantly positively correlated with overjet and significantly negatively correlated with overbite. These findings suggested that in the control group, the “high-angle” participants may have taken fewer chews per bite. In the patient group, participants with a longer mandibular body and a greater anteroposterior discrepancy between the upper and lower jaws had a faster chewing rate (chews per minute), and those with a smaller overjet and larger overbite leaned further forward while eating. Given that the number of chews was significantly smaller and mealtime was significantly shorter for participants in the patient group compared with those in the control group, it can be inferred that the participants in this group, who had large discrepancies between their upper and lower jaws and upper and lower front teeth, may not have chewed their food fully. They may have increased their chewing rate by reducing mealtime and encouraged tongue elevation by leaning further forward to swallow the larger particles formed as a result of insufficient mastication. The relationship between masticatory behavior and maxillofacial morphology thus differed between the normal and patient groups, which suggested that the patient group may have both characteristic masticatory behavior and maxillofacial morphology, and that this masticatory behavior may be linked to their maxillofacial morphology. However, as overjet is a potentially important limiting factor in the results of this study, in the future, we intend to further increase the number of participants and make comparisons.
The test food used in this study was a single standard 100-g rice ball. This was chosen so that eating implements such as chopsticks or a spoon would not affect bite size and because the number of chews used to eat a single rice ball is reportedly weakly correlated with the number of chews when eating daily meals [8]. However, there are limitations to the determination and assessment of a large number of masticatory behavior-related items using just a single food, and further studies to evaluate masticatory behavior using test foods with different physical properties, mass, and forms are required in the future.
Studies of mastication have identified sex differences in mastication ability [20]. Both the patient and control groups compared in the present study therefore had equal sex ratios. A number of points have also been raised with regard to the association between mastication and health, and in children in particular, chewing fewer times has been shown to have adverse effects, including weight gain from overeating [21]. Developmental deficiency of oral function in childhood has also been reported to result in the risk of obesity during adolescence [22]. In the present study, the mean BMI of the patient group tended to be higher than that of the control group, but it is possible that in addition to the masticatory behavior of chewing fewer times and for a shorter time, the younger mean age of this group may also have affected their BMI. Future studies should include a larger number of participants to investigate the effects of age and sex differences on masticatory behavior.
It has previously been reported that the occlusal contact area is significantly smaller in patients with mandibular prognathism than in normal participants [13]. In the present study, however, the occlusal contact area was almost identical in both the patient and control groups, with no significant difference between them. This may have been because unlike that previous study, in the present study, the control group consisted of participants with individual normal occlusion who had completed dynamic treatment, including some who had undergone tooth extraction. Given that masticatory behavior is habitual, the results for masticatory behavior obtained from the control group in this study may have reflected the persistence of characteristics acquired prior to orthodontic treatment. Future comparative studies of participants with no history of orthodontic treatment are therefore required.
In a previous study, individuality normal occlusion without previous orthodontic treatment was selected as the control group [13]. However, when these participants were selected as the control group, it was not possible to take lateral cephalograms due to radiation exposure, and patients who had acquired a unique individual normal occlusion by orthodontic treatment alone were selected as a control group and analysed and compared using the lateral cephalograms taken at the end of orthodontic treatment. Patients with orthodontic treatment alone were selected because the group of patients who had achieved individual normal occlusion by orthognathic surgery may have still had the same functional discrepancies in the stomatognathic system that is characteristic of patients with mandibular prognathism. In addition, participants with less anterior–posterior and horizontal discrepancies in maxillofacial morphology were selected because of the possibility that significant discrepancies in maxillofacial morphology could affect masticatory behavior. Based on the above, it is considered that a correct comparison could be made between patients with mandibular prognathism, which is considered to have a large discordance in maxillofacial morphology and function, and a control group. However, it is unclear whether the control group in this study had the same masticatory behavior as those who were born with individual normal occlusion. Therefore, it is necessary to compare the masticatory behavior before and after orthodontic treatment and to examine whether the correct masticatory behavior was acquired by orthodontic treatment intervention in the future.
Masticatory training is conducted after orthognathic surgery with the goals of long-term postoperative stability of the dentition and occlusion, as well as functional improvement, but objective assessment may be lacking, and many issues concerning the verification of functional improvement remain to be resolved. It would provide good motivation for patients by means of visual feedback on their masticatory behavior. It also has the potential to promote changes in masticatory behavior and contribute to habilitation with the new oral and maxillofacial morphology achieved by orthognathic surgery.







Comments (0)