The results of the present study reveal the difficulties and the necessity of the dental treatment of intellectually disabled patients. Acute treatment is costly as separate rooms, dentists, and general anesthesia are needed to perform it. That is, such treatment is more costly and more difficult to carry out, than the treatment of the general population. According to surveys, the more serious the condition and the higher the age of the patients, the more decayed teeth they will have. In view of the above, it is clear that prevention, which can be successful based on proper education, is of utmost importance. Prevention, therefore, should reach out to a broader circle of patients.
Based on the surveys conducted on the treatment of patients with intellectual disability, there is an agreement in the literature regarding the kind of anesthesia required. Patients with intellectual disabilities who cannot receive treatment under local anesthesia should instead be treated under general anesthesia [4,5,6,7]. The literature emphasizes the benefits of antiplaque agents and professional hygiene treatments to reduce gingivitis and supports that this is crucial for the prevention of oral diseases [9,10,11, 14]. In the case of patients with intellectual disabilities, the deficit in oral hygiene cannot be explained solely by the lower motivation and capability to maintain sufficient oral hygiene. Risk factors such as the caretaker’s lack of motivation and knowledge in delivering oral hygiene, oral deformities, and socioeconomic status play an important role in the oral hygiene deficit of this patient group of special needs [8, 11,12,13].
In Hungary, approximately 100,000 patients have intellectual disability, with dental treatment being administered to them under general anesthesia only. Within the 5-year study period, approximately 1800 patients required acute treatment in Budapest. Regarding patients with intellectual disability, the provision of acute interventions primarily under general anesthesia has been proposed [5, 6]. While evaluating the findings related to Semmelweis University, we discovered that similar results were evident in another center dedicated to treating patients with intellectual disabilities in Hungary, albeit with a smaller patient population [22].
Notably, some dentists aim for full-mouth rehabilitation (extraction, restorations, and dentures) during general anesthesia. However, this results in a longer duration of anesthesia and a lower number of patients being treated (Solanki et al. [7] reported 200 cases in 10 years). Furthermore, these patients should be removed from their usual surroundings for a minimal period [5, 6, 23, 24]. Additionally, intraoperative, and postoperative complications related to anesthesia should be considered. Despite the significantly higher number of interventions in our study, no patient had nose hemorrhage because the intratracheal tube was not inserted through the nose. Only a few cases of desaturation and emesis were observed.
Of the 2000 patients treated at our institution, 90% required further restorative or prosthetic treatment. The prevalence of caries in the standard population in Hungary [2] is higher than that of most European populations (DMF-T score: 3.3 in Hungary [20, 25,26,27,28] vs. 0.8 in the Netherlands [29]). Comparing the dental status of the standard population with that of patients with intellectual disability who have a high DMF-T score of 3.3 would ultimately produce an even poorer comparative score. Notably, no survey regarding the dental status of patients with intellectual disability has been published in a Hungarian scientific journal, although this could provide objective data. However, several studies worldwide have compared the dental status, relevant anatomical formulas, jawbones, and temporomandibular joints between these patients [30,31,32,33].
Iszmailov [13] examined 171 patients with intellectual disability and reported that 34% of the patients develop periodontal problems at the age of 18–25 years, whereas 82% develop periodontal problems after the age of 42 years. Mac Giolla Phadraig et al. [34], in the framework of the “Delphi panel,” determined the dental care that could be performed in patients with intellectual disability. They highlighted 16 consensual findings regarding personalized treatment, information flow, training, and costs. The most important findings referred to the buildings, equipment, and personnel involved in providing treatment. Notably, some countries have demonstrated limited progress. In an initial step, Waldman et al. [35] determined that the nationwide need for dental treatment of patients with intellectual disability should be established based on research and followed by the establishment of centers where dental treatment (including restorative dentistry and prevention), excluding the treatment by general practitioners and psychiatrists, would be available.
The number of patients requiring more than acute care exceeds the available capacity (institutions, dentists, and financial resources). Therefore, prevention should be prioritized. Notably, several prevention methods have been documented, with the results reported by Edwards et al. [8] in 2002 being the most significant. In Merseyside County (Liverpool area, mid-West England), dentists were invited to provide treatment for patients with intellectual disability. Training programs were organized for patients and their relatives to improve oral hygiene. These programs resulted in a considerable decrease in the number of patients requiring acute dental treatment and an improvement in the dental status of patients [36, 37]. Even though acute dental treatment modalities for patients with intellectual disability have recently improved in Hungary (approximately 3,000 patients were treated at five centers during the last 5 years), opportunities for complex dental rehabilitation remain limited [2].
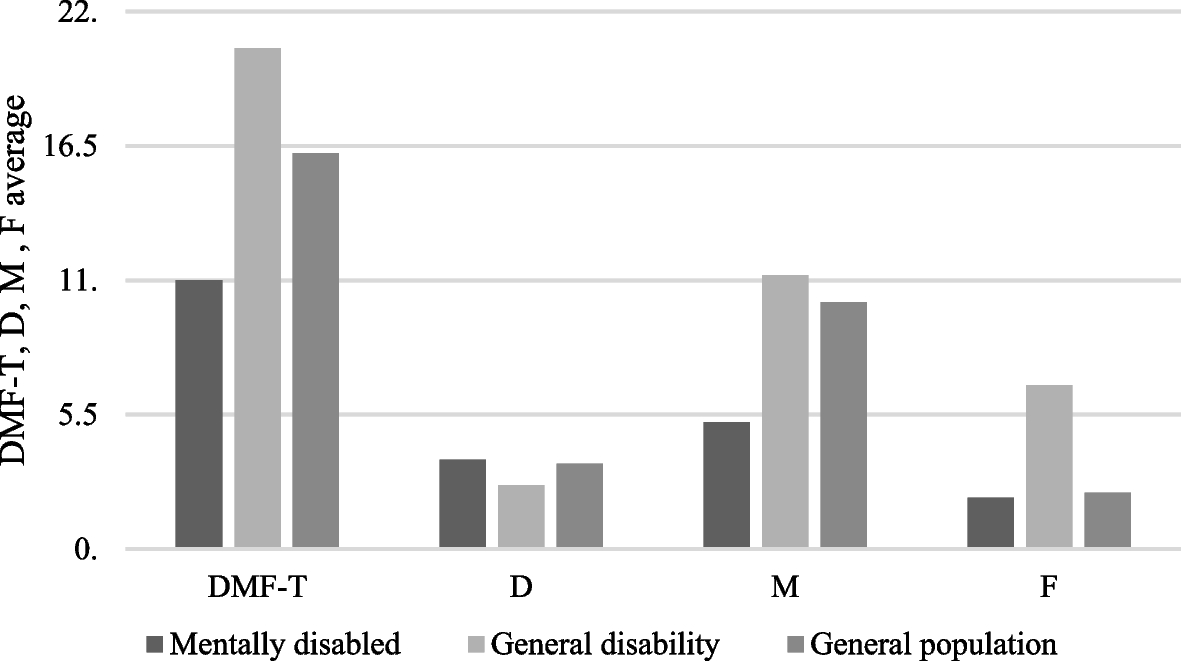
Our screening research included > 300 patients, consistent with the sample size in previous studies: 225 in India [36] and 221 in Germany [38, 39]. We originally aimed to compare the dental status of patients with intellectual disability with that of the general population; however, we also compared our findings with data pertaining to individuals with a general (mainly physical) disability (Fig. 1) [39,40,41,42]. The mean DMF-T score of the general population (4606 examined patients) was 16.2, whereas that of patients with a general disability (608 patients) was 20.5. In 325 patients with intellectual disability, the DMF-T score was 11. When comparing the dental status of patients with intellectual and physical disabilities and the general population, we found that patients with intellectual disability had the highest number of decayed teeth and the lowest number of filled and missing teeth [20, 21].
We compared the dental status of patients with intellectual and physical disabilities and the general population in an age group of 20–44 years because 85% of the examined patients were in this age group. For patients with intellectual disability and those in the general population aged ≤ 19 years, the mean (± standard deviation) DMF-T score was 6.09 ± 7.13 and 11.24 ± 4.85, respectively; in the age group of 20–34 years, it was 9.21 ± 6.33 and 12.76 ± 5.45, respectively; and in the age group of 35–44 years, it was 11.91 ± 6.77 and 15.40 ± 5.13, respectively. To understand this apparent paradox, we need to simplify the DMF-T score. Patients with intellectual disability had the highest number of decayed teeth (D = 3.7). Providing dental treatment to such patients is complicated because most require general anesthesia; therefore, the most frequent intervention is extraction (M = 5.2). Restorative treatment is rarely performed (F = 2.2). In the general population, F, D (lowest), and M were 2.3, 3.5, and 10.1, respectively. In patients with general disabilities, M was 11.2.
Providing dental treatment to patients with intellectual disability is challenging. Therefore, preventive measures should be applied as widely as possible. In the United States, treatment of patients with special needs (including those with intellectual disability) is a part of the curriculum at several universities [43]. Comparing the toothbrushing habits of healthy children and those with intellectual disability of the same age [44], patients with intellectual disability pay less attention to their teeth than healthy children. Therefore, in terms of prevention, patients with intellectual disability need enhanced care. In the United States [45], children with intellectual disability (those born in the 1990s) were examined and educated in the presence of their parents before school about the importance of cleaning their teeth and maintaining oral hygiene. Follow-up examinations performed subsequently showed that the dental condition of these children was considerably better than that of other children needing special care.
The survey by Boyle et al. [46] indicates that the prevalence of patients with intellectual disability in the United States is approximately 6.7/1000. Due to poor oral hygiene, 90% of these patients develop periodontal diseases [47]. According to Wyne [48] in a study in Pakistan, most patients with intellectual disability have periodontal diseases because of inadequate oral hygiene and not due to their basic condition. Notably, Hungarian authors [49, 50] have reported the general and dental conditions of patients with physical disability and have recommended the implementation of special programs accordingly [51,52,53,54].
A limitation of this study was the small sample size enrolled in the preventive care program which limits the generalizability of its findings. However, the sample size was sufficient to prove the feasibility of the preventive program for patients with intellectual disability. A further limitation regarding the comparison of the DMF-T scores of the intellectually disabled patients to that of the general population and population with general disability was that a multivariate analysis could have accounted for some confounding factors (e.g.: socioeconomic status or access to care).
The findings of control examinations performed after 3 or 6 months did not reveal any apparent improvement in the present study. This was not unexpected, as the interval of 3–6 months is too short to observe any progress in the reduction of caries incidence. Relying on our proposed relatively simple training program, we showed that the scope of our work should be widened. Improved dental care and enhanced (normal) oral hygiene maintenance can result in substantial changes in a relatively short period. The attitude of the caretakers and parents toward the program is important. The first phase of rehabilitation is the survey of needs; the second is the implementation of prevention procedures; and the third, which is the most difficult and expensive, is performing adequate surgical and/or restorative treatments. The first phase is complete, whereas the second, as reflected by the current prevention program, is underway. The third phase, as far as acute treatments are concerned, is partially complete; however, in the field of restorative dentistry, limited progress is evident, with prevention programs playing a significant role.
The retrospective study results on acute treatments for patients with intellectual disabilities indicate that it is crucial to enhance funding for facilities offering this type of treatment and to establish more centers. Furthermore, it is crucial to implement preventive training programs in nursing homes to improve the oral hygiene of patients with intellectual disabilities and reduce the need for invasive surgery under general anesthesia.







Comments (0)