
Remember me






According to the results of this study, no significant differences were observed in the degree of improvement of the subjective symptoms of patients experiencing xerostomia-associated mucositis due to their prescribed medication, hormonal imbalance, and Sjögren’s syndrome. These results suggest that for these patient groups, NBF gel without pilocarpine might be sufficient to improve subjective symptoms of constant xerostomia-associated mucositis and glossodynia inter cibos. However, NBF gel did not stimulate saliva secretion. Thus, supplementing NBF Gel with pilocarpine is necessary to avoid dysphagia.
NBF Gel was launched in South Korea in early 2008 [26, 27]. NBF Gel is a highly functional gel, created for the first time by a process where nanotechnology is fused with biotechnology [26]. The result is the creation of a nano-emulsion composed of ultra (nano) particles of vitamin C, vitamin E, and propolis extract. The mouth is naturally a moist environment; thus, the contact time of topically applied medicine is limited. The nanoparticles of vitamin C, vitamin E, and propolis extract overcome this problem due to their ultra-fine size [25, 28, 29]. They are much more efficient in rapidly penetrating the cells than their regular size counterparts [21]. Once applied, the NBF gingival gel creates a film that results in increased absorption, improved clinical potency, and decreased toxicity. The gel does not contain either alcohol (no burning effect) or benzocaine (numbing effect) [26, 27].
Since 2008, we have been using the cream at the NBF Gel prescribed at the Department of Oro-Maxillofacial Surgery and Stomatology, Semmelweis University since 2008 [21]. In our previous study, we reported on its application in 68 patients. NBF Gel was used successfully in the treatment of various oral lesions, including post-operative lesions, particularly following laser surgery, diseases of the oral mucosa (aphthous ulcers, herpes, leukoplakia, lichen, glossodynia, ulcers during chemotherapy, etc.) [21]. The international literature also reports favorable results in cases of gingivitis, chronic periodontitis, desquamative gingivitis, erosive lichen planus, and diabetic lesions [23, 24, 28, 30,31,32,33,34,35,36].
In the medical literature, the treatment of gingival diseases often involves antibiotics and non-steroid anti-inflammatory drugs (NSAIDs) [37]. However, oral medications frequently have systemic side effects, and topical medications are usually ineffective as they are difficult to retain in the mouth [11, 16, 19]. Thus, using an effective local agent that facilitates healing is justified. The NBF Gel is rapidly absorbed at the cellular level and is competitive with all products used for local oral mucosa treatment [21, 25, 38].
Returning to the various causes of xerostomia, the consequences of salivary gland damage or just functional loss are not straightforward. During the radiation treatment of head and neck tumors, radiation damage to the maxillofacial area occurs even if the patient wears a protective mask during the treatment, albeit to a lesser extent [5, 7, 39, 40]. The result of irradiation is the destruction of glandular cells and the proliferation of fibrotic tissues in the glandular parenchyma [5]. Even if the remaining glandular tissue function is stimulated, the drying of the oral mucosa occurs, partly because the radiation directly damages the mucosa, and partly because the serous glands do not produce sufficient saliva despite stimulation [41]. Chemotherapy has similar effects as irradiation [40, 42, 43]. During treatment, ulcers may form in the mouth in addition to xerostomia, for which the NBF Gel is excellently suitable [21].
In the case of Sjögren’s syndrome (benign lymphoepithelial lesion), lymphocytes destroy epithelial cells in the ductal system of the salivary glands, resulting in dilations and small bullae in the fine primary salivary ducts where the damaged epithelial cells used to be [6, 44]. These bullae accumulate saliva, which can become retrogradely infected. Repeated inflammations further damage the glandular tissue [6, 44]. Therefore, a two-way treatment is important: enhancing saliva secretion (pilocarpine) and locally treating the dry mucosa (NBF Gel). In this way, the patients’ objective symptoms improve, and the subjective dry, sometimes burning sensation (glossodynia) greatly improves [21].
In the case of hormonal and drug-induced dry mouth, the neurohormonal balance necessary for normal saliva secretion is disrupted [10, 18, 45,46,47]. In the serous glands, the basal membrane surrounding the salivary-producing cells acts as a filter: sympathetic stimuli reduce its permeability (from the glandular cells to the primary salivary ducts), while parasympathetic stimuli expand the filter, allowing saliva to be discharged from the glandular cells [48].
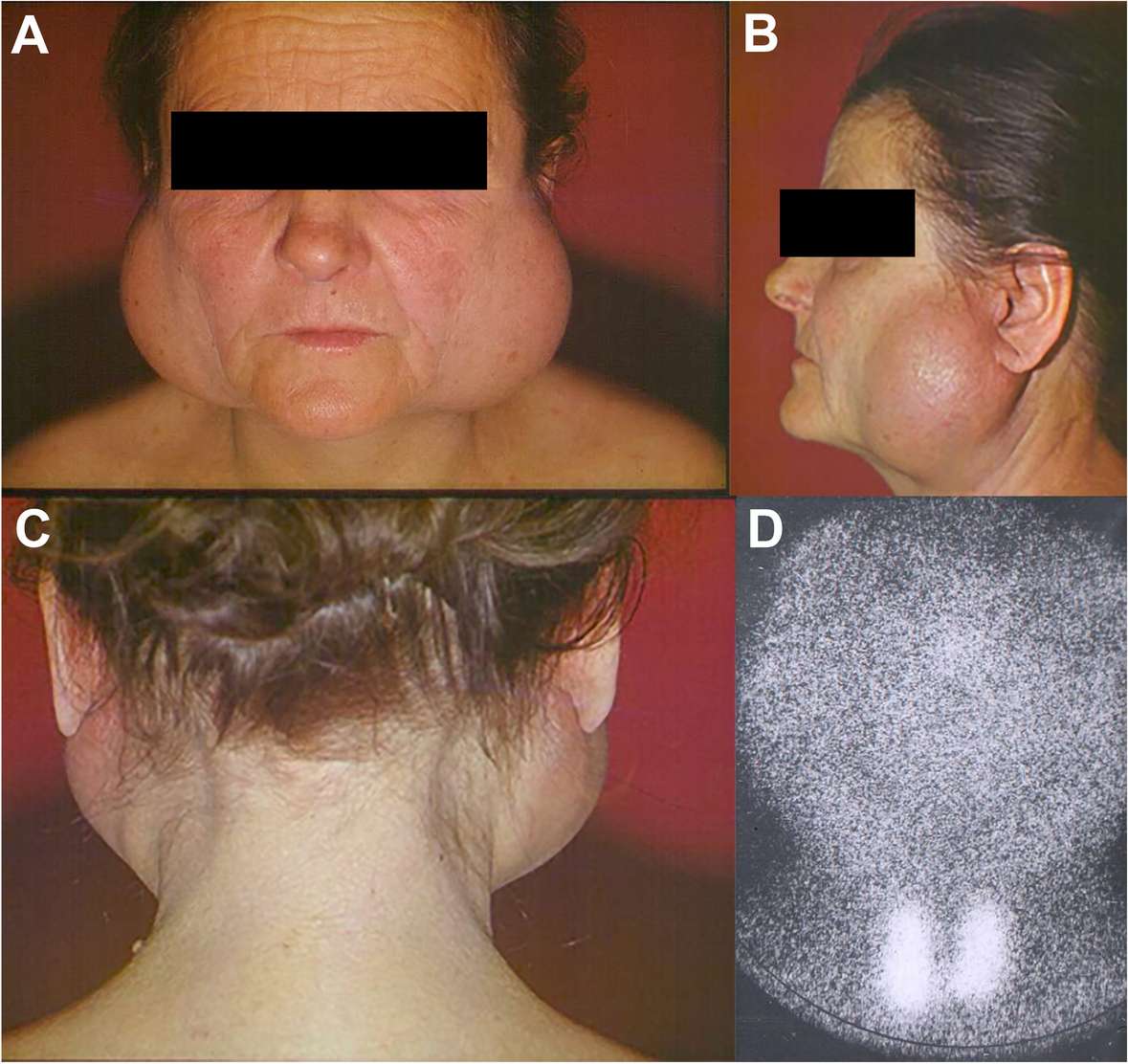
Due to its composition, the NBF cream does not improve salivation. While the cause of xerostomia-associated mucositis is the lack of saliva, the associated symptoms—such as the subjective feeling of constant dry mouth, glossodynia, oral mucosal ulcers that appear after irradiation or chemotherapy, and difficulties in swallowing during eating—are alleviated by the NBF cream [21]. Pilocarpine may be prescribed to enhance salivation, and the NBF cream complements its effect by improving subjective symptoms of xerostomia. In this study, pilocarpine and NBF cream were prescribed together. Therefore, in the present study, the effectiveness of the cream was measured by changes in the subjective feelings of the patients. There is no objective measure described in the literature for changes in the subjective comfort of xerostomia patients. In severe cases of post-irradiation xerostomia and Sjögren’s syndrome, where there is practically no functioning salivary gland tissue remaining, even with the aid of pilocarpine, it is impossible to produce more saliva. The clinical manifestation of a severe case of Sjögren’s syndrome is presented in Fig. 1. In these cases, the NBF Gel becomes even more significant as it provides the most favorable treatment for the dried-out mucosa.
Fig. 1
Presents the clinical features of a severe case of Sjögren’s syndrome with major lymphoid infiltration, without any remaining salivary gland tissue (A, B, and C). Salivary glands are not visible on the scintigraphy (D), only the thyroid gland
Despite demonstrating promising results, this study has several limitations that should be considered when interpreting the findings. First, the study did not include a negative control group, meaning we could not directly compare the outcomes of the NBF Gel-treated group with a completely untreated group. However, we mitigated this limitation by comparing the condition of patients before and after NBF Gel treatment. In this context, the pre-treatment state served as a baseline equivalent to a “no treatment” group, allowing for some level of comparative analysis. Second, the study primarily relied on subjective measurements, such as the Visual Analogue Scale (VAS), to assess the effectiveness of NBF Gel. While subjective assessments are crucial for understanding the patient’s experience and perceived improvements, they may introduce biases or inconsistencies due to individual differences in perception and reporting. Incorporating objective measurements, such as the clinical evaluation of mucosal healing or quantitative assessments of mucosal thickness and integrity, could provide a more comprehensive understanding of the treatment’s effectiveness and reduce potential subjectivity. Third, although the study observed a reduced dosage of pilocarpine when used in combination with NBF Gel—resulting in fewer side effects—this finding was not compared to a group receiving pilocarpine alone. A direct comparison between the NBF Gel and pilocarpine combination group and a pilocarpine-only group would be necessary to better understand the additive or synergistic effects of NBF Gel on reducing pilocarpine dosage and its associated side effects. These limitations highlight the need for future studies to include negative control groups, incorporate both subjective and objective measurements, and compare combination therapies to monotherapies to strengthen the evidence for the clinical benefits of NBF Gel in treating xerostomia-associated mucositis.
Comments (0)