
Remember me





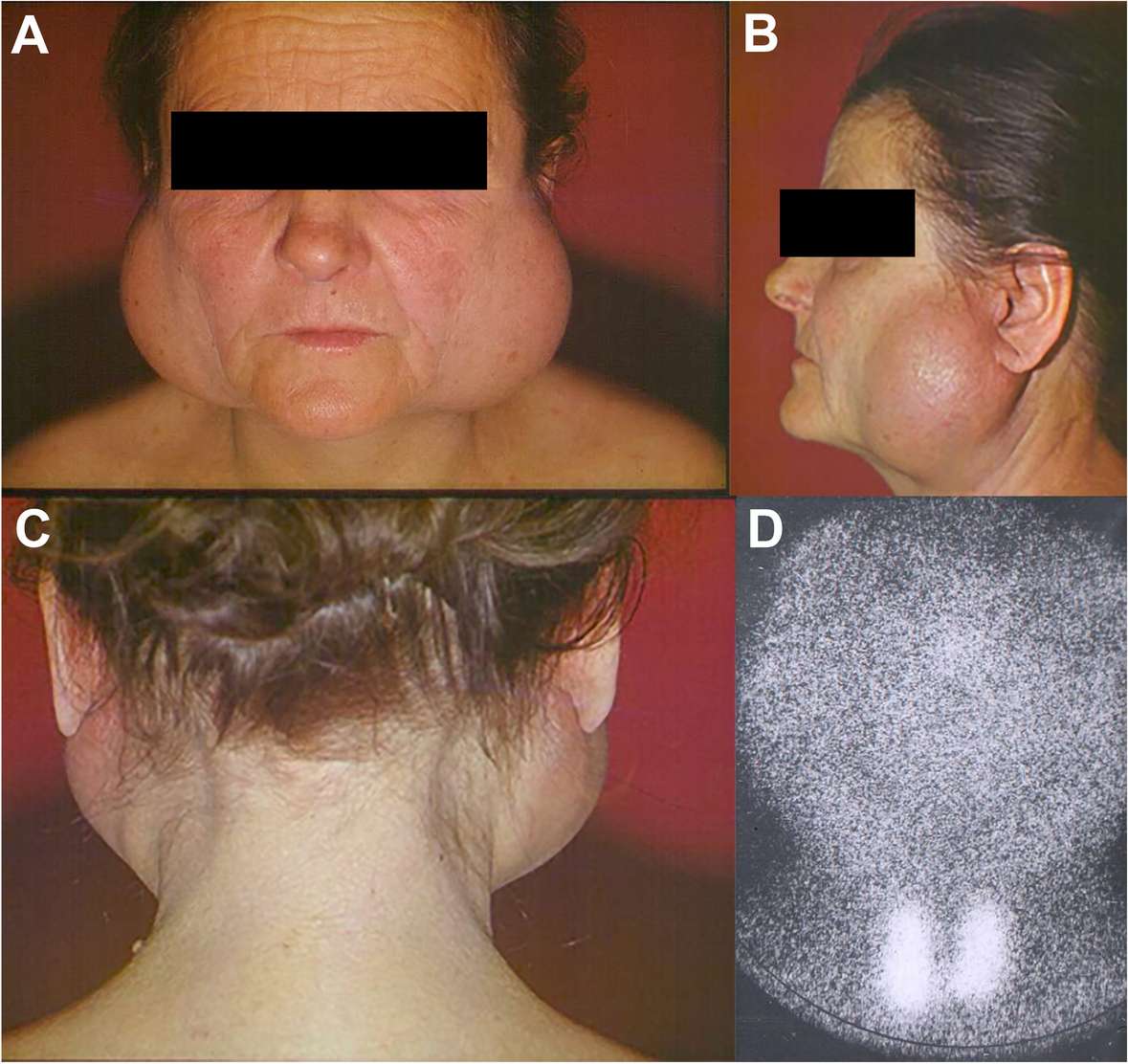

A 16-year-old female patient presented with a congenital facial anomaly characterized by bilateral Tessier 3 and Tessier 0 clefts (Fig. 1). Clinically, the patient exhibited significant nasal deformity with the absence of the nasal septum, widened nasal dorsum, and increased distance between the alae nasi, consistent with the features of a median cleft. Additionally, the patient displayed hypertelorism and midfacial flattening, with a wide intercanthal distance. The maxillary region showed asymmetry with malocclusion and dental crowding, along with a defect extending to the lower eyelids and orbital rim. Despite the severity of the anomaly, the patient had no significant history of systemic illness or prior surgical intervention. A comprehensive evaluation, including 3D CT imaging, confirmed the extent of the craniofacial defects, highlighting the challenges in reconstructive planning. Comprehensive 3D computed tomography (CT) imaging revealed significant craniofacial anomalies, including complete absence of the nasal septum, widened interorbital distance measuring 38 mm (consistent with hypertelorism), and cranial displacement of the alae nasi. The maxillary region displayed asymmetry with malocclusion and crowding of teeth. These imaging findings provided critical insights for surgical planning, confirming the extent of bony and soft tissue involvement and the need for a staged reconstructive approach. This case demonstrates the unique combination of rare facial clefts, requiring a multidisciplinary approach for functional and aesthetic restoration.
Fig. 1
Clinical and radiological manifestations of bilateral Tessier 3 and Tessier 0 facial clefts. A Preoperative frontal view showing bilateral Tessier 3 and Tessier 0 clefts with significant cranial displacement of the alae nasi, widened nasal dorsum, and hypertelorism. B Lateral preoperative view highlighting the absence of nasal septum and flat midfacial profile. C 3D computed tomography (CT) reconstruction illustrating the complete absence of the nasal septum, widened interorbital distance measuring 38 mm, and asymmetry in the maxillary region. These findings provided critical information for surgical planning and highlighted the complexity of the reconstruction
The bilateral Tessier 3 cleft in this patient presented with several unique and complex anatomical features, setting it apart from typical cases. One of the most notable characteristics was the malposition of the alae nasi, which were displaced cranially, far from their normal anatomical location. This cranial displacement significantly altered the nasal appearance and structure, creating both functional and aesthetic challenges. Additionally, the patient exhibited an unusual configuration of the nasal openings. There were two visible nasal passages: an upper opening that was blind-ended and non-functional, and a lower opening that was the sole pathway used by the patient for breathing. This abnormal configuration not only affected nasal airflow but also posed challenges for surgical correction and functional restoration.
This study was conducted in accordance with the ethical standards of the institution, and IRB approval was not required as it is a single case report. Written informed consent for publication of their clinical details and/or clinical images was obtained from the patient. A copy of the consent form is available for review by the Editor of this journal.
The surgical reconstruction was performed in three stages, with a 6-month interval between the first and second stages to ensure proper soft tissue healing and stabilization. The first stage prioritized establishing a functional nasal airway and repositioning the alae nasi to improve nasal alignment. The second stage focused on reconstructing the absent nasal septum and restoring nasal contour using costal cartilage grafts. A final stage involved dorsal refinement and medial repositioning of the alae nasi to optimize nasal symmetry. This sequential approach minimized surgical risks such as cartilage warping and tissue necrosis, allowing for gradual adaptation of nasal structures.
The first surgical intervention was meticulously planned to address these unique deformities. The primary focus of the procedure was the repositioning of the alae nasi to their correct anatomical location, moving them downward to achieve a more natural alignment with the midface. This repositioning aimed to improve both the functional and aesthetic aspects of the nose. In addition, the blind-ended upper nasal opening was surgically perforated and connected to the functional lower nasal passage. This step was critical in creating a unified and functional nasal airway, allowing the patient to breathe through the nose in a manner comparable to that of a normal individual.
The overarching goal of the surgery was twofold: first, to achieve a proper anatomical position for the alae nasi, and second, to establish functional nasal passages that would enable the patient to breathe through the nose comfortably and effectively. This surgical approach not only addressed the immediate functional issues but also laid the groundwork for future interventions aimed at further improving the patient's quality of life and nasal aesthetics. The combination of these unique anatomical features and the complexity of the surgical correction highlights the challenges and innovations required in managing rare craniofacial anomalies like bilateral Tessier 3 clefts (Fig. 2).
Fig. 2
First-stage surgical reconstruction: alae nasi repositioning and airway creation. A Surgical design and markings outlining the repositioning of the alae nasi and creation of a functional nasal airway. B Intraoperative image demonstrating cranial displacement of the alae nasi and the blind-ended superior nasal opening. Partial excision was performed to create an opening that could be connected to the functional lower nasal passage. C Immediate postoperative result showing successful repositioning of the alae nasi to their anatomical location and the establishment of a unified functional nasal airway, allowing effective nasal breathing
In the subsequent stage of surgery, the primary focus was on addressing the Tessier 0 anomaly, specifically reconstructing the absent nasal septum. This was achieved by creating an L-shaped septal extension graft and a dorsal onlay graft, with the distal end of the graft meticulously positioned on the nasal bone to provide structural support and improve nasal contour. The procedure was executed as planned, and the surgical team was confident in achieving the desired structural improvements. However, during the closure process and subsequent follow-ups in the outpatient clinic, it was observed that the nasal shape was not yet optimal (Fig. 3).
Fig. 3
Second-stage reconstruction: costal cartilage grafting for septal and dorsal support. A Harvesting of costal cartilage from the right sixth rib. The cartilage was sculpted into an L-shaped graft comprising a septal extension graft and dorsal onlay graft. B Intraoperative placement of the L-shaped graft. The septal extension graft provided central support, while the dorsal onlay graft restored nasal height and contour. C Immediate postoperative appearance demonstrating improved nasal contour and projection. The reconstructed nasal septum provided enhanced structural stability, though minor asymmetry of the nasal dorsum was noted during follow-up
The primary concern noted was the imbalance in the dorsum nasi, which was caused by the significant distance between the right and left alae nasi. This disproportion created an asymmetry in the nasal structure, detracting from the aesthetic results of the reconstruction. To address this, an additional surgical intervention was deemed necessary. This involved the removal of excess soft tissue from the nasal dorsum, which had contributed to the asymmetry, and the approximation of the right and left alae nasi to reduce the interalar distance and create a more harmonious nasal shape. This stage also includes ala nasi repositioning on the medial side (Fig. 4).
Fig. 4
Third-stage refinement: medial repositioning of alae nasi and dorsal reduction. A Surgical design for medial repositioning of the alae nasi to reduce the interalar distance. Wedge excisions were planned at the alar base, and excess soft tissue was marked for removal from the dorsal nasal area to improve nasal contour. B Intraoperative image showing rotational flaps on both alae nasi for precise repositioning and dorsal tissue reduction. C Immediate postoperative outcome highlighting enhanced nasal symmetry, reduced interalar distance, and improved dorsal contour. The surgical scar was strategically placed along the dorsum nasi to minimize visibility
The secondary procedure was carefully staged to ensure the structural integrity of the reconstructed nose was preserved, avoiding overcorrection or compromising the functional outcomes. The scar from this procedure was strategically placed along the dorsum nasi, serving as a clear and defined boundary for the nasal contour while minimizing its visibility. This meticulous approach aimed to achieve both functional and aesthetic improvements, providing the patient with a more natural nasal appearance while ensuring that the structural foundation of the nose remained uncompromised. This staged reconstruction highlights the complexity of managing craniofacial anomalies and the importance of iterative surgical planning to address evolving anatomical and aesthetic considerations effectively (Fig. 4).
The current nasal appearance of the patient demonstrates significant improvement following the staged reconstructive surgeries (Fig. 5). The nasal dorsum is now relatively straight and well-defined, though minor irregularities in contour remain visible, likely due to the scarring from prior interventions. The nasal tip appears broad with limited projection, contributing to a slightly flattened appearance. The alae nasi have been repositioned symmetrically and are better aligned with the midface; however, the interalar distance remains relatively wide, which impacts the overall nasal proportions. The nasal openings are now functional and centrally positioned, enabling the patient to breathe effectively, a significant improvement from the preoperative condition. Despite these advancements, some aesthetic refinements could still be considered, particularly in improving nasal tip projection and harmonizing the overall proportions.
Fig. 5
Final postoperative appearance at 12-month follow-up. A Frontal view showing improved nasal symmetry, well-defined nasal dorsum, and symmetrical alae nasi positioning. The interalar distance was significantly reduced compared to the preoperative state, contributing to balanced facial proportions. B Lateral view illustrating adequate nasal projection and stable contour. C Basal view revealing functional and symmetrical nasal openings with a patent airway. Minor dorsal irregularities remain, primarily due to scarring from previous interventions. The patient declined further refinement procedures, including orbital box osteotomy, citing satisfaction with the current aesthetic and functional outcomes
To achieve more balanced facial proportions and create a more favorable foundation for nasal reconstruction, particularly in the dorsum nasal area, a comprehensive surgical strategy was proposed. This plan involved addressing the patient’s telecanthus and hypertelorism, which are significant contributors to the overall facial asymmetry and disproportion. The recommended procedure was an orbital box osteotomy, a complex yet effective surgical technique designed to correct the widened interorbital distance and bring the orbits into a more anatomically harmonious alignment. This correction would not only improve the aesthetic symmetry of the face but also provide a more stable and proportional base for subsequent nasal reconstruction.
Despite the potential benefits of the orbital box osteotomy in enhancing both functional and aesthetic outcomes, the patient expressed concerns regarding the high risks associated with the procedure. Due to its invasive nature and potential complications, the patient ultimately declined this intervention. This decision highlights the delicate balance between achieving optimal surgical outcomes and respecting the patient’s preferences and tolerance for risk. The surgical team remains committed to exploring alternative approaches that align with the patient’s goals while maintaining safety and minimizing potential risks. This case underscores the importance of individualized treatment planning in complex craniofacial reconstruction.
Comments (0)