Corynebacterium species are endemic to the conjunctival sac and are not highly pathogenic [20,21,22]. Therefore, when Corynebacterium species are detected in ocular infections, it is important to determine whether they are pathogenic or not. In this study, we focused on cases with a strong suspicion of infectious keratitis based on clinical findings, in which Corynebacterium species were solely identified from corneal scrapings and therefore considered pathogenic. To the best of our knowledge, this is the first review of Corynebacterium keratitis in Japan and the first study that has examined the shape of lesions in multiple patients.
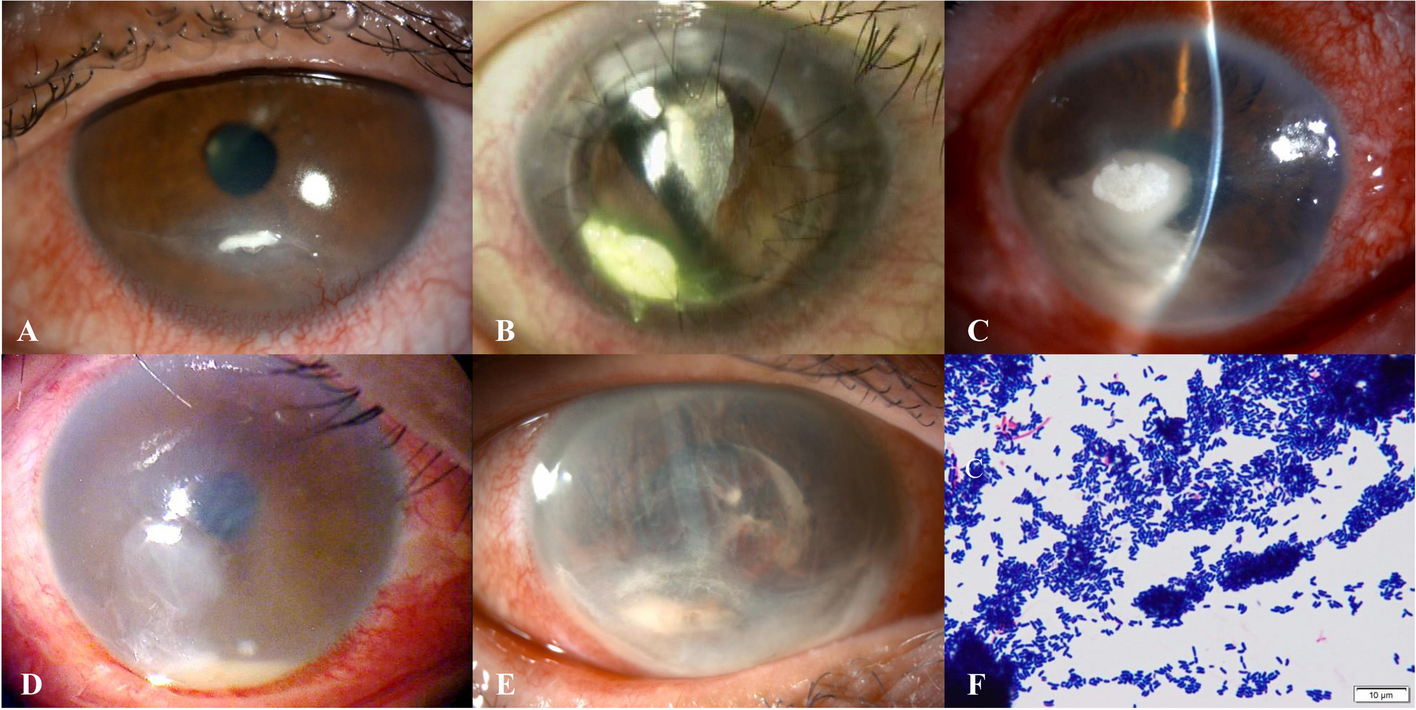
In this study, the clinical findings of keratitis caused by Corynebacterium species were classified into two types: adherent and infiltrative (Fig. 1). Gram staining of the adherent material revealed numerous gram-negative rods. This suggests that Corynebacterium species may adhere to the corneal surface layer, formed a bacterial colony, and produced a biofilm. Corynebacterium species adhere to biomaterials such as catheters and corneal sutures and form biofilms [8, 23]. On the other hand, Mihara et al. reported a case in which Corynebacterium species adhered to the scleral cornea and formed a biofilm and colonies [24], suggesting that Corynebacterium species may form colonies on the ocular surface without biomaterial.
The major risk factors for Corynebacterium keratitis are reportedly ocular surface disease [13, 17] and contact lens use [15]. In this study, ocular surface diseases such as dry eye and lagophthalmos and contact lens use were also recognized as risk factors. Soni et al. also reported that the use of steroid eye drops was an important risk factor [17]. Similarly, in this study, the use of steroid eye drops was observed in more than half of the patients. Furthermore, 30.4% of our patients had diabetes mellitus. Corynebacterium species are attenuated bacteria [20]. Thus, a deficiency in ocular and systemic immunity may be important triggers for Corynebacterium keratitis. Eguchi et al. reported that C. macginleyi, clinical ophthalmic isolates, is highly resistant to fluoroquinolones [25]. Suzuki et al. reported two cases of keratitis due to C. macjinleyi that were induced by long-term use of fluoroquinolone eye drops after corneal transplantation [8]. In this study, the predominance of fluoroquinolone-resistant Corynebacterium species on the ocular surface due to the selective pressure by the use of fluoroquinolone eye drops could have contributed to the development of Corynebacterium keratitis.
In our study, all patients with a history of herpetic keratitis or lagophthalmos exhibited an adherent lesion. In lagophthalmos and decreased corneal sensation due to herpetic keratitis, blinking decreases, which may facilitate the adhesion of Corynebacterium to the corneal surface and contribute to the formation of the adherent lesion. Further studies are required to determine the triggers that contribute to lesion formation.
In our study, MALDI-TOF MS revealed that 85.7% of the causative organisms were C. macginleyi. In a report by Hoshi et al. 84% of Corynebacterium species isolated from the conjunctival sacs were C. macgileyi [26]. Sagerfors et al. reported 29 cases of keratitis in which C. macginleyi was identified [15], and Suzuki et al. reported two cases of keratitis caused by C. macginleyi [8]. Based on the results of our study and those of previous studies, C. macginleyi may be a major Corynebacterium species that is endemic on the ocular surface and a causative agent of keratitis.
In this study, the drug susceptibility of the isolated Corynebacterium species was high. However, the resistance rate to any of the fluoroquinolones was 91%, with C. macginleyi strains demonstrating a 100% resistance rate. Reports of Corynebacterium keratitis from other countries have stated a resistance rate of 0% to 58.3% to fluoroquinolones among the Corynebacterium species, which is much lower than that in our study [13, 15, 17]. Corynebacterium species do not possess topoisomerase IV, and only DNA gyrase mutations cause resistance, making Corynebacterium species more likely to become resistant to fluoroquinolones [27, 28]. Therefore, the overuse of fluoroquinolones in Japan may have resulted in more Corynebacterium species becoming resistant to this antimicrobial. In the present study, C. macginleyi that was highly resistant to levofloxacin (MIC > 32 µg/mL) was detected in 14 of 15 isolates (93.3%). Furthermore, 10 of these isolates had an MIC ≥ 128 µg/mL. Eguchi et al. found that a double mutation of amino acids 83-S and 87-D of GyrA in the DNA gyrase of C. macginleyi induces highly resistance to fluoroquinolones [25]. It is possible that the strain identified in this study also had a double mutation of the GyrA amino acid.
In the present study, topical cefmenoximes were widely used. Cefmenoxime is a third-generation cephalosporin with a broad spectrum of activity against both gram-positive and gram-negative bacteria. It is particularly effective in ocular infections because of its good penetration into ocular tissues and low resistance rates among ocular pathogens. However, cefmenoxime is not widely available in many regions. Thus, potential alternatives, such as cefazolin (a first-generation cephalosporin) and vancomycin (a glycopeptide), which are also effective against gram-positive bacteria including Corynebacterium species, should be considered. In previous reports, Corynebacterium keratitis has been treated with topical cephalosporins [8,9,10, 12, 29]. The isolates in this study showed good susceptibility to cephalosporins, with a resistance rate of 0%. Considering these results, in cases of infectious keratitis, when Corynebacterium species are suspected as the causative pathogen based on patient background, clinical findings, and gram staining microscopy and culture of corneal scrapings, fluoroquinolone treatment should be avoided, and cephalosporins should be used instead.
None of our cases required therapeutic keratoplasty. In contrast, previous reports showed that 8.3% to 18.2% of patients required keratoplasty [13, 17]. It is possible that frequent use of topical cephalosporins from the beginning of treatment in almost our cases may have been effective. Some of our patients with adherent type required frequent corneal scrapings. Corynebacterium species have been reported to generate biofilms on the ocular surface and form plaques, which are clusters of bacteria [8, 24]. Because bacteria in biofilms are resistant to antimicrobial agents [30] and can evade the host immune response [31], adherent lesions, which are clusters of biofilm-covered bacteria, may be difficult to treat with conservative therapy. Thus, physical removal of the bacteria may be useful for treatment.
Our study has several limitations. First, it was a relatively small, retrospective, single-center study with a limited sample size. More extensive studies are required to characterize the clinical features in detail. Second, the mechanisms underlying the development of the two types of keratitis remain unclear. In vivo models of Corynebacterium keratitis need to be established to study the factors involved in the pathogenesis of keratitis.








Comments (0)