Contact lens-related keratitis is considered a major problem all over the world and it is responsible for significant visual loss among contact lens users [5, 16]. In our study the prevalence of CLNK and CLMK was 20.4%, and 18.8% which is considered a high percentage compared to studies published by Lam et al, Stapleton et al , and Poggio et al as they estimated the incidence of contact lens-related keratitis at 2 to 20.9 per 10 000 lens wearers per year [4,5,6]. This is attributed to the nature of the study participants who were seeking medical advice in our hospital. Female gender predominated (96.0% of CLNK cases and 95.7% of CLMK cases). These results were consistent with those reported by Bin Yousef et al (95.8%) [17]. Females are more affected because they use soft contact lenses more than males either for cosmetic or refractive purposes. Regarding age, the mean age in the studied groups was 27 and 30 years, respectively. This was close to the mean age published by Wu et al. (33.8 years) and Dart et al. (32.3) [18, 19]. Oliveira et al. reported younger mean age (23.5 years) since 71% of the participants were university students [20]. The CLAY study results suggest that CL wearers between ages 15 and 25 are at increased risk relative to ages between 8 and 15 years old, this may be attributed to those adolescents and young adult have lower compliance with contact lens hygiene recommendations [21].
Our study analyzed CLK specific risk factors for each of microbial and non-microbial keratitis in contact lens wearers separately including two inadequately studied risk factors; sharing lens and eye trauma. Sharing contact lenses was a risk factor in 16% and 21.7% of CLNK and CLMK cases, which was also reported previously in Saudi Arabia (16.6%) [22]. This percentage was higher than Jordanian university students where sharing CLs accounts only for (1%) [23, 24]. This difference may be attributed to the difference in study participants’ hygiene and culture. Eye trauma before or during wearing contact lenses is another inadequately studied risk factor. An alteration or defect in the epithelial cell layer of the cornea in the presence of a sufficient number of pathogens can lead to CLMK and that was confirmed with our results where coexisting eye trauma was a significant risk factor for both CLNK (p=0.001) and CLMK (p=0.017).
Interestingly, our study showed that overnight wear of contact lenses increased the risk of CLNK. Similarly previous studies [25, 26], discussed the effect of overnight wear of lenses as a risk factor to CLK. Oxygen diffusion is compromised during sleeping leading to corneal hypoxia. Both extended CL wear and overnight CL wear were associated with the presence of IL-8 and epidermal growth factor both of which lead to CLNK [27]. Regarding CL wear duration for more than 12 hours, we found an increased risk of CLNK in the studied group. These results were not similar to Lubis et al. and Young et al. who reported that CLNK was not correlated with daily lens wear duration, but it was affected by many factors such as contact lens material, lens care solution, eye drops usage, and environment [28, 29]. Moreover, Urgacz et al. reported the occurrence of ulcerative keratitis and superficial punctate keratitis due to the hypersensitivity to preservatives in contact lens care solutions [30]. This is a limitation in our study since we did not investigate contact lens material, lens care solution, and eye drops usage as risk factors to CLK. This point is of importance and needs further research.
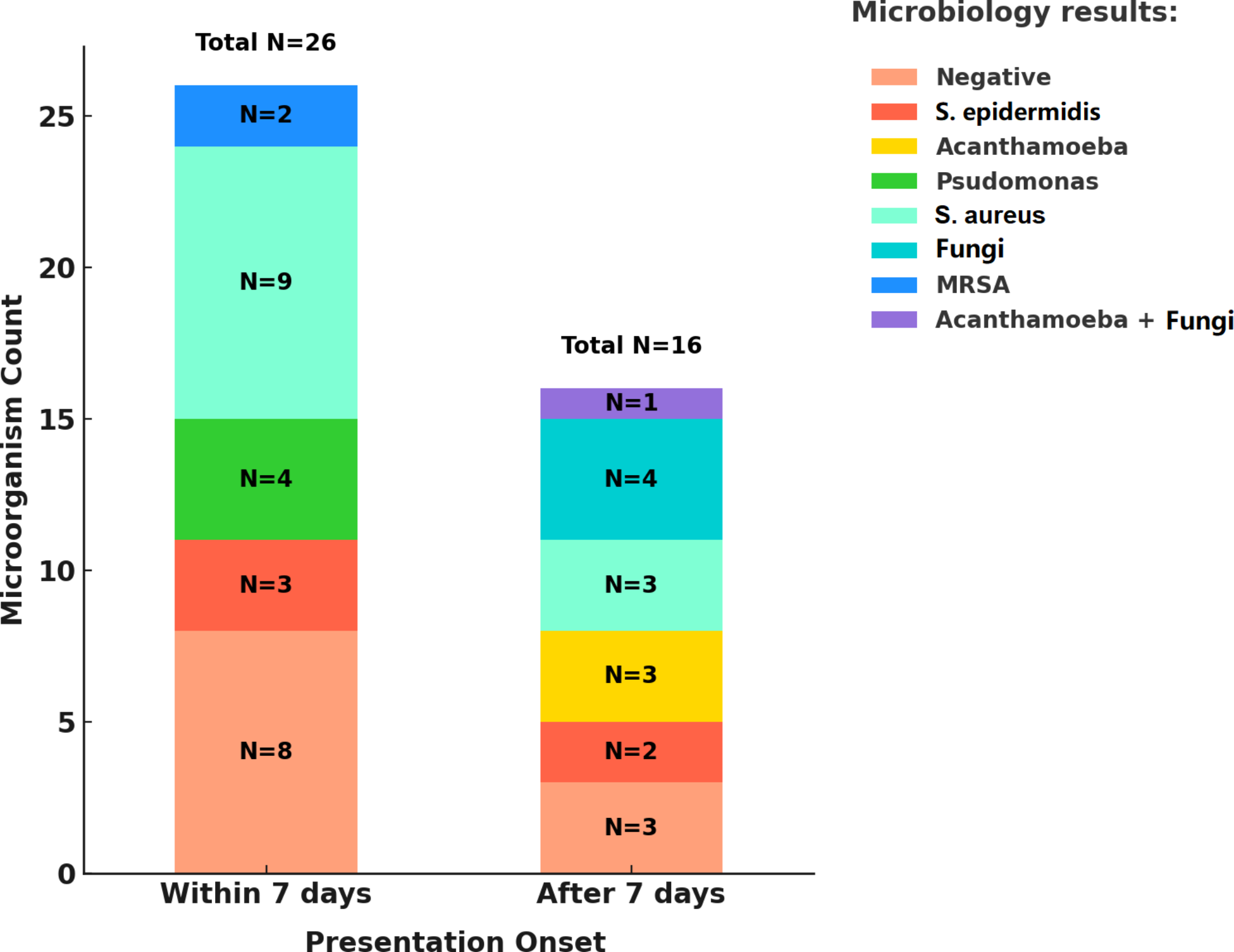
In our study, showering or swimming while wearing lenses and washing lenses with tap water significantly increased the risk of CLMK. Acanthamoeba was the most prevalent causative organism to CLMK in our study (47.8%), and this value is higher than that published in the literature by Otri et al (16.9%) [31]. Zhang et al. estimated AK incidence globally, India has the highest incidence at 15.2 cases per million per year, followed by New Zealand, Egypt, Portugal, and the UK (5.2, 5.0, 4.5, and 4.3 cases per million per year, respectively) [32], this variations may be attributed to alterations in sociocultural, environmental, and climate conditions, along with differences in contact lens prescribing practice, eye care availability, and the unawareness of CL wearers of the recommended hygiene procedures, especially regarding water exposure. Acanthamoeba cysts and trophozoites are present in air, dust, soil, and fresh water. They are highly resistant to disinfection with chlorine and are thus not eradicated from tap water [11, 33]. Al-Herrawy et al. isolated Acanthamoeba spp. from finished water samples in Egypt [34]. Moreover, acanthamoeba spp. have been identified in CL or CL cases; variable contamination rates have been verified in different geographic regions; 53.3% in Egypt [15], 15.1% in Korea [35], 10% in Iran [36] and 65.9% in Spain [12]. For this reason, showering or swimming with contact lenses, washing contact lens with tap water all can be considered risk behaviors to acanthamoeba keratitis. Fungi represented only 2.2% of positive scrapes. However, the incidence of fungal keratitis is much higher in India (23–36%) since these microbiological agents are more frequent in tropical and subtropical regions than in temperate regions [37, 38].
Our study showed that 88.0% of CLNK cases and 93.5% of CLMK cases washed their hands before touching lenses, which is similar to that reported from studies in Saudi Arabia (71.9%), and (89.4%) [22, 39]. A lesser percentage was reported from Maldives (44.2%) [40]. This discrepancy may be due to differences between target populations and hygiene practices.
CL purchases by internet order [5] or at unlicensed cosmetics shops [41] were reported to increase the risks of adverse events because these places never provide eye examinations and/or sufficient counseling. Although our results were not consistent with these findings, we emphasize the need to control purchasing CLs from unlicensed stores.
Contact lenses…. are designed for visual and cosmetic purposes, but instead of the visual correction that they were originally invented for …. now accused of causing significant keratitis and visual impairments due to multiple risk factors. CLNK is thought to be one of the predisposing factors to CLMK which is not fully studied and this needs future research.
The strengths of our study are the precise results acquired by face-to-face interviews using a standardized questionnaire and the confirmed diagnosis done clinically by cornea team consultants and laboratory by microbiological investigation.
The findings from this research support the mission of public health ophthalmology which aims to create awareness of adverse events related to CL and to improve CL user behaviors to maintain their health and safety. All CL users should reduce daily wear time by avoiding overnight wearing, and avoiding water exposure. Campaigns are considered a practical solution to contact lens-related keratitis prevention indeed. The study provided updated guidelines to CLMK for healthcare providers for proper management and better outcomes. Eye professionals should follow guidelines regarding CLK diagnosis and management and advise all CL users about regular eye examination and lens hygiene.








Comments (0)