In contrast to prior studies limited to evaluating IVCM for detection and diagnosis of AK often in relation to other diagnostic methods, the present investigation was a RWD study aimed at highlighting how IVCM examinations have been incorporated into clinical practice at a regional referral center for IVCM. While the retrospective study design and focus on a single center revealed incompleteness of information prior to arrival or after discharge from the referral center, a major strength of the study is that it highlights the use of IVCM in handling suspected AK cases in a real-world setting outside the controlled conditions of a clinical study, where special measures are made to obtain as complete datasets as possible. Most prior studies also report a short follow-up duration for patients, without clear timelines for AK resolution. In Sweden in particular, the only published series involving AK (but not IVCM) describes 8 patients treated over 30 years ago [15]. Given the escalating usage of contact lenses and the increasing incidence of AK cases in recent years, assessing the current real-world diagnosis and treatment of patients with suspected AK in centers with IVCM is essential. This study highlights key areas for improvement in the integration of IVCM into a clinical setting where multiple hospitals may refer patients to a single regional referral center with expertise in IVCM.
Overall, our referral center examined 81 suspected AK patients in a 12-year period with IVCM. Not all cases were well-documented, likely because patients were sometimes referred for the sole purpose of performing an IVCM examination and reporting results to the home clinic. For referrals from another hospital requesting a second opinion, half were IVCM-positive and treatment was initiated at our referral center, with the other half being IVCM-negative and directly returning to the care of the home clinic. These cases could be followed up with the referring clinic in the future, to better understand the clinical outcomes related to the IVCM-based diagnoses.
A large group of referred patients had IVCM-negative and inconclusive findings, and of these cases many were bacterial keratitis. For those cases not treated at our center, future follow-up to determine the final diagnosis would aid in evaluating the features observed by IVCM. Regardless of patient category in this study, however, most patients received some form of care at our center prior to discharge or return to the home clinic. The median time of care and number of visits to our center were highly variable but were generally extensive. Typically, the management of patients with suspected AK lasted years, not months, with the entire group of patients having a median of 11 clinic visits during the study period, which does not include prior or subsequent visits at the home clinic. The group with the longest median management time (about 6 years) was the referred to our center for a second opinion and subsequently managed at our center. These were cases of delayed diagnosis or misdiagnosis, and/or treatment-resistant cases with repeated sequelae and co-morbidities, where patients often underwent multiple surgical interventions with long follow-ups. This illustrates the complexity of managing AK cases in the real-world setting, and the significant clinic resources allocated to this patient group. Nevertheless, we found a significantly shorter time of care and fewer clinic visits for IVCM-negative cases relative to IVCM-positive cases. Moreover, 100% of IVCM-negative cases who had culture samples taken were also culture-negative, representing a 100% negative predictive value for IVCM at the referral center. This highlights that IVCM examination can successfully predict those cases which are likely not AK and will thus have a shorter clinical course and require fewer resources.
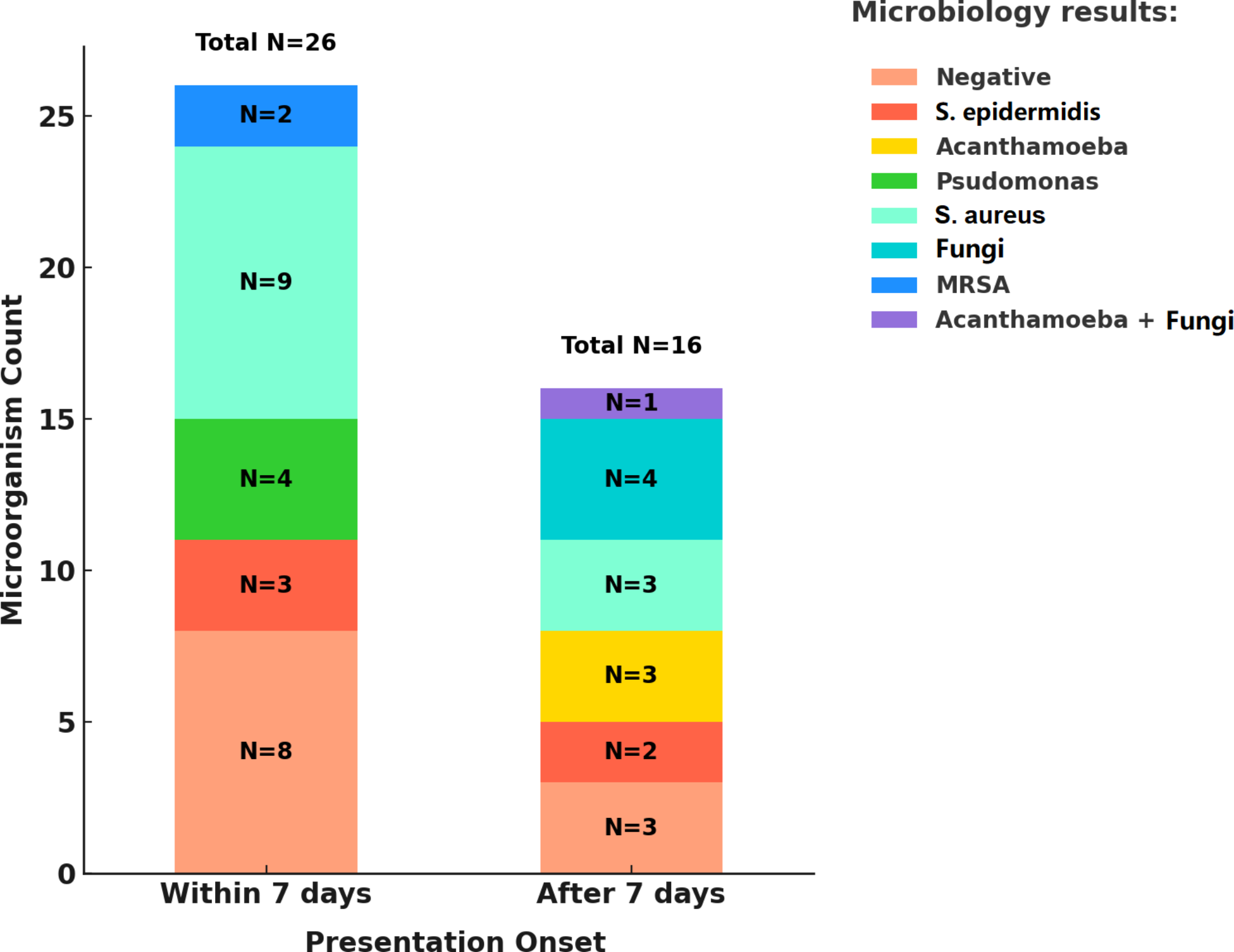
While 57% of the population were documented contact lens wearers, the proportion may have been higher as the etiology was not systematically recorded in the patient charts. Ideally, all patients with suspected AK would also, in addition to IVCM, have samples taken for culture and/or PCR. This reflects the different practices at different centers and in different countries, and the real-world situation where not all diagnostic modalities may be available, or where time may be of the essence, particularly with a patient receiving a positive diagnosis then returning to the referring clinic. Even where multiple diagnostics are available, the treating physician may choose not to employ all of them, particularly where IVCM indicates a clear positive result or where resources are limited. At the referring centers and at the IVCM referral center during the time frame of this study, PCR was not implemented as a diagnostic technique (but has later been adopted at larger academic centers in Sweden), and cultures were taken in only about half of the cases at the referral center, in contrast to controlled studies evaluating the diagnostic accuracy of IVCM, which have typically shown a good diagnostic accuracy [4], although this can be dependent on the level of experience of the IVCM operator [21]. In the real-world setting at our center, a positive IVCM finding resulted in the patient immediately receiving anti-amoebic therapy without culture samples typically being taken. Also, culture was performed mostly in cases not responding to first-line pharmacologic treatment. In these cases, the clinical picture, patient history/predisposing factors and IVCM findings were sufficient for initiation of treatment. The typically long delay in receiving culture results and typically low culture positivity for AK may have also played a role in the decision not to take a culture sample. On the other hand, a negative IVCM finding often resulted in either a transfer back to the referring center or in some cases a culture sample being taken. Reliance on culture results was not high at our center, and this may partly be due to the finding that only 2 cases were culture-positive for AK whereas 22 cases were IVCM-positive for AK. Moreover, half of the culture samples were negative for pathogens of any kind. Drawbacks of the culture method have previously been shown in other studies, possibly due to the culture sample not containing any cysts [20, 22]. It may also be possible that the culturing method used may not be adequate or that previous applied therapies may impede the ability to culture the parasite. Time constraints also play a role as cultures typically require a time frame of 2 days to 2 weeks, and the proportion of positive results varies widely, ranging from 0 to 68%, which is also a major disadvantage [23, 24].
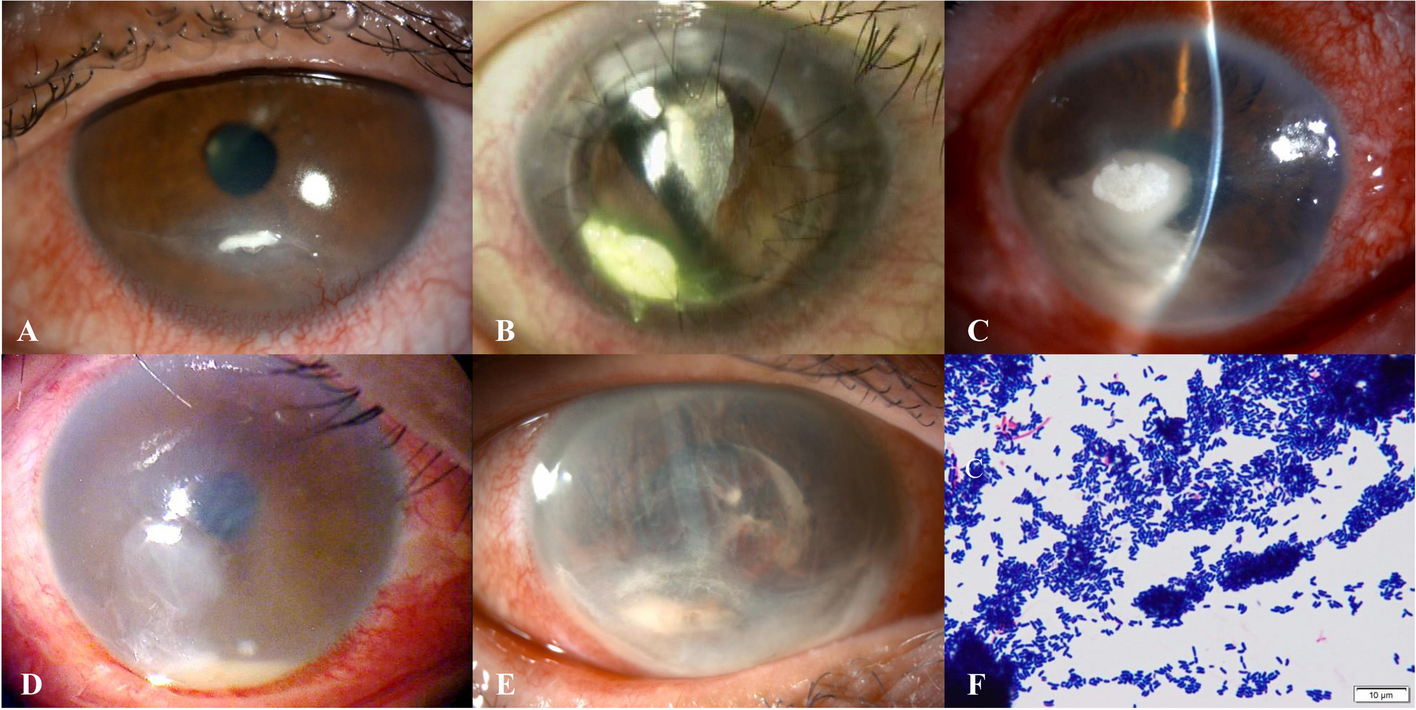
Evaluation of images from IVCM-positive cases always revealed cysts on at least one visit (100%), and additionally dendritic cells (88.9%) and a clear inflammatory infiltrate (66.6%). It should be kept in mind, however, that cyst identification is done by humans, and although machine learning tools are being developed [25], a risk for false positives remains [20]. The analysis indicated that patients returning to their home institutions exhibited more severe inflammation (P = 0.04) and worse corneal nerve status (P = 0.004) at their final IVCM examination at our referral center compared to those remaining under care at the referral center until resolution. This likely reflects the active infection and inflammation still present upon discharge, which is expected to improve with continued patient management at the home clinic. It is important to note that the presence of cysts in repeated IVCM examinations does not necessarily indicate therapy resistance or lack of improvement, as the activity of these cysts could not be determined. Previous studies have shown that infection resolution does not always eliminate cysts [8, 26, 27]. Therefore, an integrated assessment of all clinical characteristics is necessary to determine the clinical significance of findings of residual corneal cysts.
The relatively long time of care in this study was often the result of a long patient history prior to referral to our center, often characterized by multiple prior diagnoses, and for this reason the study may be biased towards reporting the most difficult and complex cases. These cases, however, are those typically sent to our regional referral center, which is part of an academic hospital. In Sweden (with a population of 10.5 million), only 4 centers are currently using IVCM. Unfortunately, delayed initiation of appropriate treatment can have a significant impact on prognosis, as it has been reported that starting treatment after one month of symptom onset leads to greater morbidity and poorer visual outcomes [28]. A study involving 105 AK patients showed that early diagnosis resulted in a final visual acuity of 6/12 or greater in over 90% of cases, while delayed diagnosis resulted in this level of vision in only 65% of cases [29]. In addition, more advanced deeper infections are ten times more likely to be associated with poorer VA [5] and the need for subsequent surgical interventions [30]. Therefore, a possible solution could be a centralized approach to manage suspected and diagnosed AK cases at a single center experienced in the use of IVCM. This would require better education and outreach to the referring centers that do not use IVCM.
Notably, we did not find differences in VA from the first to the final patient visit at our center, regardless of the patient category. This may be due to the high proportion of severe keratitis cases referred to our center, where vision improvement is often secondary to the eradication of the causative pathogen. VA measurements, however, also constitute a limitation in our study. Aside from lack of complete visual acuity data in all patients, acuity values in the patient records were measured by different physicians often with varying levels of accuracy. Ocular comorbidities impacting vision further complicate the representation of VA as an outcome measure of AK treatment.
In this study we identified a subgroup of 14 patients (19%) who visited the clinic for a single IVCM examination with the sole purpose to confirm or rule out AK diagnosis. It is important to note that relying on a single examination may not capture pathognomonic features such as cysts, particularly in the early stages of the disease when a dense inflammatory infiltrate may be present. Moreover, a previous study highlighted the advantages of follow-up IVCM examinations [8], where the density of cysts during the early stages of the disease can be minimal, with the highest density occurring approximately two weeks after initiating AK treatment, followed by a clear reduction after about 2 months of treatment. This peak in cyst numbers is attributed to the two-cycle life form of Acanthamoeba, where trophozoites convert into cysts in response to the treatment-induced unfavorable microenvironment. Therefore, only a short-term assessment of patients could lead to erroneous conclusions and suboptimal management including unnecessary surgery [8]. Longer term evaluation with IVCM may serve as a reliable indicator of the patient’s responsiveness to AK treatment, based not only on cysts but on other signs of healing such as regeneration of subbasal nerve fibers, resolution of the inflammatory infiltrate, healing of the ulcer (return of epithelial cell mosaic), and a lower grade of dendritic cells.
The results of this study also suggest a clear need for better documentation since information can be transmitted verbally between treating centers and may not be adequately documented in the medical record system (for example, with a formal referral letter) when patients are referred. Moreover, the medical record system in Sweden is region-based; to obtain full patient history and outcomes for patients outside the region of the referral center would require specific research ethics, collaboration and data sharing agreements across multiple regions and hospitals. Additionally, relying on a single IVCM examination may prove insufficient in ruling out an AK diagnosis, instead multiple examinations are desirable. Follow-up of patients with repeated IVCM examinations, while highly variable in this real-world setting, could in the future be better prioritized and standardized.
Given the results and limitations of this study, we recommend the following measures to be taken by referral centers for IVCM in Sweden receiving suspected AK cases:
1.
A comprehensive system for monitoring and recording clinical information from patients with a positive IVCM diagnosis for AK across referring and referral centers is needed; if this is hindered by different region-based systems and regulations on data sharing, an alternative is to develop a national registry for AK-positive cases. In this way, all information regarding the AK diagnosis and treatment for patients would be available in a single place, regardless of which clinics or regions the patient visits.
2.
Not all cases of suspected AK are examined with IVCM. It is recommended that upon suspicion of AK, regardless of whether a culture sample or swab is taken, the patient is referred for IVCM examination. Given the many clinic visits and long time to resolution for AK, the benefits would likely outweigh the extra cost for referral, given that AK is a relatively rare but potentially devastating condition. This recommendation may involve targeted outreach and communication to clinics where IVCM is not available.
3.
Strict protocols should be implemented for documentation of contact lens wear and other risk factors in patient records in cases of suspected and confirmed AK.
4.
Upon detecting positive evidence of AK by IVCM, referral centers should communicate the preferred treatment regime to the treating physician, which is of particular importance when patients return to the home clinic for subsequent management. Consistency of first-line treatment regimens could improve outcomes.
5.
Referral centers should take culture and PCR samples in addition to performing IVCM, if the referring center had not initiated these complementary diagnostics.
6.
In cases of positive IVCM diagnosis, the referral center should recommend further follow-up visits for IVCM even if the patient returns to the home clinic for medical management.
In summary, to the best of our knowledge, this is a unique real-world study evaluating all suspected AK cases referred for IVCM during a 12-year period. IVCM had a 100% negative predictive value that also mirrored a shorter clinical course to keratitis resolution and coincided with positive culture detection of other pathogens in these AK-negative cases. Importantly, positive IVCM detection of AK was much more frequent than culture positivity for AK. Direct instatement of anti-amoebic medical therapy upon positive IVCM findings led to AK resolution in many cases, although the time to resolution was long, given the advanced nature of AK and long clinical history of patients seen at the regional referral center. Additionally, a group of suspected AK cases were inconclusive by IVCM, which is an important group and highlights the practical limitations of IVCM and the continued need for multiple clinical diagnostics and follow-ups in cases of suspected AK. Improved communication and information sharing between referring clinics and the referral center could yield benefits for patients by potentially reducing the time to diagnosis and aiding in ongoing patient management. Standardization of documentation and diagnostic routines in the management of AK, as well as spreading of information across regions about IVCM as an available diagnostic method could also yield improved care for patients and better exploitation of the utility of IVCM as a complementary diagnostic tool in a real-world context.








Comments (0)