This retrospective study presented the incidence rate, features, and outcomes of infectious keratitis following PRK in a tertiary hospital over a 13-year period.
In our center, the post-PRK infectious keratitis incidence rate was reported as 0.018%. which was within the range reported in former studies (Table 6) [9,10,11,12,13].
Table 6 Incidence of post-PRK infectious keratitis in different studiesThere is debate concerning the rate of infectious keratitis after photorefractive surgeries when comparing PRK and LASIK [14, 15]. Rojas et al. reported a 5.7-times higher incidence rate of infectious keratitis in patients undergoing surface ablation compared to those undergoing LASIK [15]. The same group [16] reported a decrease in the incidence of post-PRK infectious keratitis from 0.2 to 0.066% when tobramycin and moxifloxacin were used as prophylactic topical antibiotics compared to tobramycin alone; nevertheless, their incidence was 6 times higher than after LASIK (0.011%). This difference has been attributed to factors such as corneal epithelial defects, the use of bandage contact lenses, and corticosteroids used for managing the wound healing process in PRK cases [17, 18]. However, a recent meta-analysis study demonstrated that the incidence rate of keratitis was 4.5 times lower after PRK compared to LASIK [14]. The higher frequency of LASIK procedures and the creation of a corneal flap have been proposed as potential explanations for this observation [14, 19]. Taken together, infectious keratitis remains a significant complication following both PRK and LASIK, highlighting the need for optimizing prevention and management strategies to minimize the risk of adverse outcomes [15, 19].
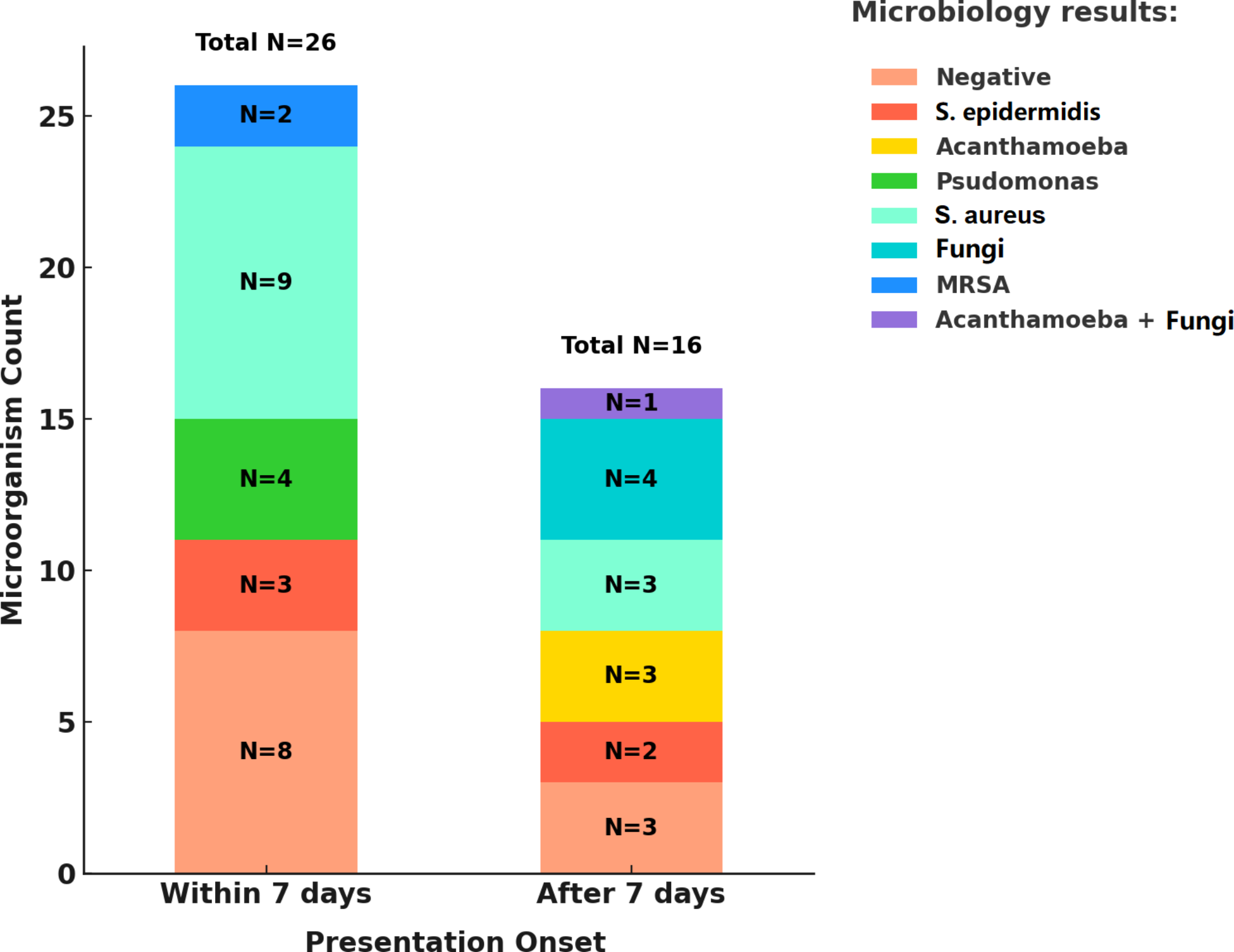
The presentation time of infectious keratitis following photorefractive surgeries is important in determining its type and may help clinicians make appropriate practical decisions [8]. In our study, 61.9% of cases were classified in the early-onset group. Similarly, it has been reported that approximately 50–60% of infectious keratitis cases present within the first week following surgery, emphasizing the importance of careful monitoring during this period [20,21,22]. It has been reported that early-onset cases are typically caused by bacteria such as Staphylococcus, Streptococcus, and Pseudomonas, while late-onset cases are often due to slow-growing organisms such as Mycobacteria, Nocardia, Acanthamoeba, and fungi [22, 23]. These findings are consistent with our results.
Regarding the involved eye, Soleimani et al. found that the incidence rate of post-PRK infectious keratitis was higher in the left eye [9]. The time passed since ocular prepping was hypothesized as an explanation for their finding [9]. Similarly, in our study, all cases underwent PRK in the right eye at first. However, the rate of keratitis was higher in the right eye. Therefore, further prospective studies on this matter are recommended.
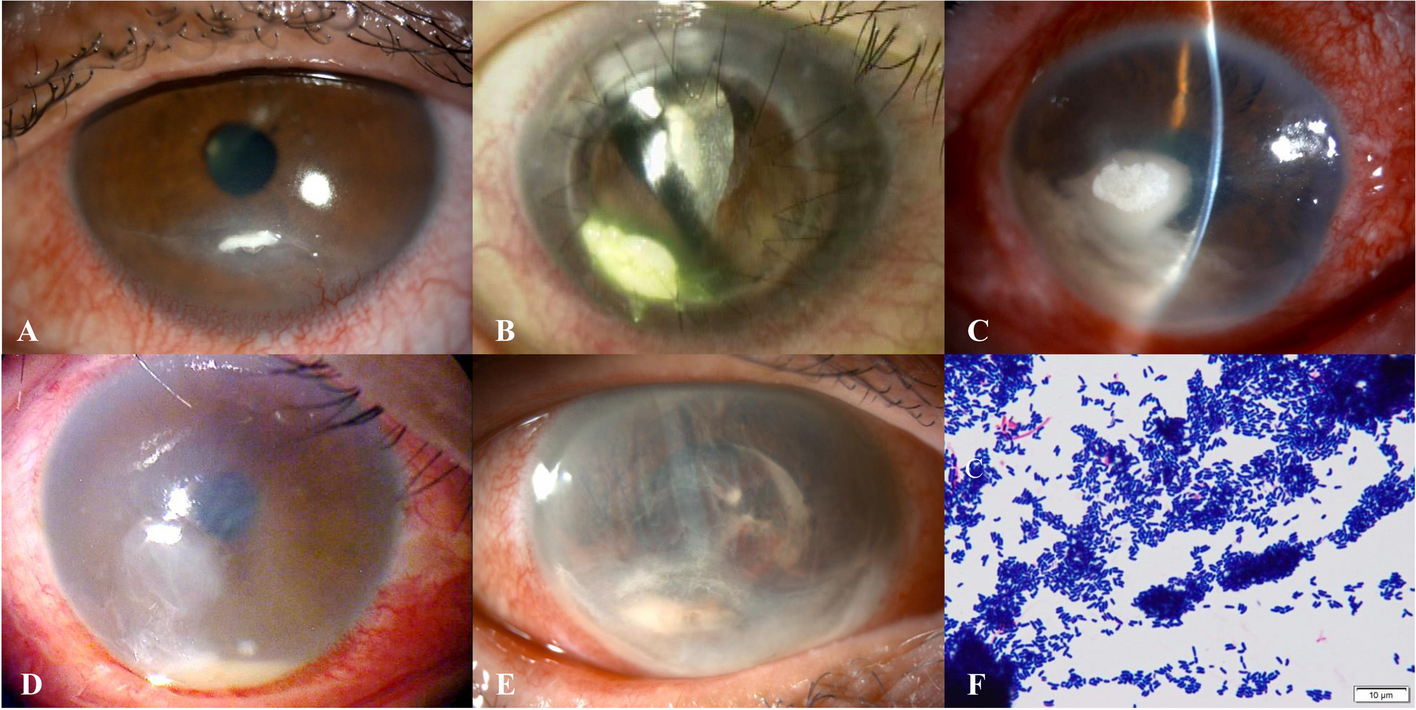
Patients with post-PRK infectious keratitis typically present with clinical symptoms such as decreased CDVA, eye pain, photophobia, redness, discomfort, discharge, and excess tears [8, 9]. In the initial assessments, corneal infiltrations, epithelial defects, ciliary injections, and hypopyon may be diagnosed [8, 9].
In suspected post-PRK infectious keratitis cases, a culture study of the contact lens and corneal scraping should be performed for accurate diagnosis [24]. The infiltrate in cases of post-PRK infectious keratitis is easily accessible for sampling [20]. Most organisms can be identified through Gram staining and Blood agar cultures. However, in cases with late-onset, it is desirable to also use Ziehl-Neelsen staining, Lowenstein-Jensen media for mycobacteria, and Sabouraud dextrose agar for fungi [25].
Our findings are consistent with previous studies, which identified gram-positive microorganisms as the most common causative agents of post-PRK keratitis [9, 26, 27]. Therefore, prophylactic antibiotics against gram-positive bacteria after PRK have been recommended [9]. No cases of mycobacterial infection were identified in our study. This aligns with previous studies, which have reported that unlike LASIK, surface ablation procedures are rarely related to postoperative atypical mycobacterial infections [9, 24, 28].
Several risk factors for infectious keratitis following PRK, such as contact lens manipulation, dry eye, healthcare professional, blepharitis, ocular trauma, diabetes, frequent hospital encounters, contamination during surgery, and use of corticosteroids have been reported [8]. We identified blepharitis, dry eye, diabetes, swimming in the sea, manipulation of contact lenses, ocular trauma, exposure keratopathy due to previous blepharoplasty, washing with water, healthcare-related work, and bandage contact lens (BCL) dislodgment as possible predisposing factors.
Hence, a thorough ophthalmic examination before the surgery and managing dry eye and blepharitis is essential [24]. The use of the SPEED Questionnaire for ocular surface diseases may help ophthalmologists in identifying these conditions prior to surgery [29].
Studies on contact lens-related keratitis have shown a high prevalence of Pseudomonas aeruginosa induced keratitis [30]. These findings align with our results, which showed that 50% of cases of Pseudomonas aeruginosa infection had a history of contact lens dislodgement. Therefore, regular and frequent corneal examinations are necessary until complete healing of the corneal epithelial defect is achieved, and the bandage contact lens should be removed as promptly as possible [14].
Both MRSA-infected cases in our study were employed in healthcare facilities. This was consistent with previous studies demonstrating an increased risk of MRSA-related infectious keratitis associated with healthcare settings [26, 31].
Soleimani et al. reported that the higher use of face masks during the COVID-19 era was associated with the increased incidence of infectious keratitis following PRK surgery [32]. In their study, the risk ratio and odds ratio for infectious keratitis after PRK were 9.11 and 9.00 during the COVID-19 pandemic, respectively [32]. Similarly, in our center, the incidence of post-PRK infectious keratitis was significantly higher during COVID-19 pandemic, with a sevenfold increased risk compared to outside the pandemic. This may be explained by the redirection of airflow containing oral flora towards the eyes due to mask usage, thereby elevating the infection risk in a cornea that is already compromised [33].
According to previous guidelines, the treatment of infectious keratitis following PRK surgery involves aggressive antibiotic therapy and contact lens removal [34].
It has been suggested that fortified preparations of antibiotics, such as ceftazidime, vancomycin, tobramycin, and cefazolin, are effective against a broad spectrum of gram-positive and gram-negative bacteria [20]. Additionally, the use of topical corticosteroids should be discontinued [35]. In cases of fungal suspicion, the treatment regimen should be adjusted to antifungals such as voriconazole, natamycin, or amphotericin B [22]. Cases with keratitis caused by Acanthamoeba are suggested to be managed with topical chlorhexidine and PHMB [22].
We started fortified ceftazidime and vancomycin as empirical treatment (during hospitalization), followed by oral doxycycline (after discharge) for all the patients. Additionally, we started voriconazole/natamycin and PHMB in cases of keratitis caused by fungal and Acanthamoeba, respectively. Furthermore, linezolid was started for patients with keratitis caused by MRSA. We found that except for one patient (affected by Acanthamoeba), 97.6% of all cases with post-PRK infectious keratitis responded to antibiotic therapy. These findings were in concordance with the results of former studies by Rojas et al. [15], Ortega-Usobiaga et al. [16] and Soleimani et al. [9], who found that nearly all the cases with post-PRK keratitis responded to medical treatment.
Most lesions have been reported to resolve with medical therapy within a few weeks [25]. However, for infections that do not respond to treatment, corneal biopsy or polymerase chain reaction (PCR) may be necessary to identify the causative pathogens [36]. In addition, in severe or non-resolving cases, interventions such as corneal cross-linking or PK may be required [25, 37]. In this regard, patients who developed endophthalmitis (during their hospitalization) and patients with unresolved corneal scarring (at follow-up visits) underwent PK in our study. Notably, we found that the final CDVA of the patients who underwent PK was significantly better than the overall final CDVA of all patients.
Meanwhile, the majority of cases with keratitis caused by fungi, Pseudomonas aeruginosa, Staphylococcus epidermidis, and Acanthamoeba required PK, whereas none of the cases caused by Staphylococcus aureus, MRSA, and negative-culture keratitis required PK.
In our study, 50% of patients achieved a CDVA of 5/10 or better after follow-up. The CDVA of patients at follow-up was worse compared to the results of previous reports, which have reported a CDVA of 20/40 and 20/20 in over 90% and 50% of cases, respectively [9, 10, 15]. This variation may be due to the fact that we only evaluated hospitalized patients and did not include non-hospitalized cases, who naturally have a better initial CDVA and prognosis compared to those requiring hospitalization.
To the best of our knowledge, the present study is the most extensive investigation to date on post-PRK keratitis incidence, with regular and long follow-up periods, that may provide valuable insights for clinicians on managing infectious keratitis. However, the present study has some potential limitations. Firstly, given the retrospective nature of this study, the reported rates of infectious keratitis following PRK surgery may contain inaccuracies, as some affected patients may have sought treatment from other physicians or centers or may not have completed the follow-up period. Secondly, we only included hospitalized cases, excluding those who received outpatient treatment, which may skew the results towards poorer outcomes, and affect the reported incidence of post-PRK corneal infections. Thirdly, our culture studies included some negative results, possibly due to technical issues or prior antibiotic use. Finally, the wide 95% CI for the odds ratio (1.58 to 31.52) comparing the incidence of post-PRK infectious keratitis during and outside the COVID-19 era indicates that the results of this comparison should be interpreted with caution due to the small number of keratitis cases. Therefore, future prospective studies are needed to address these limitations more effectively.








Comments (0)