
Remember me

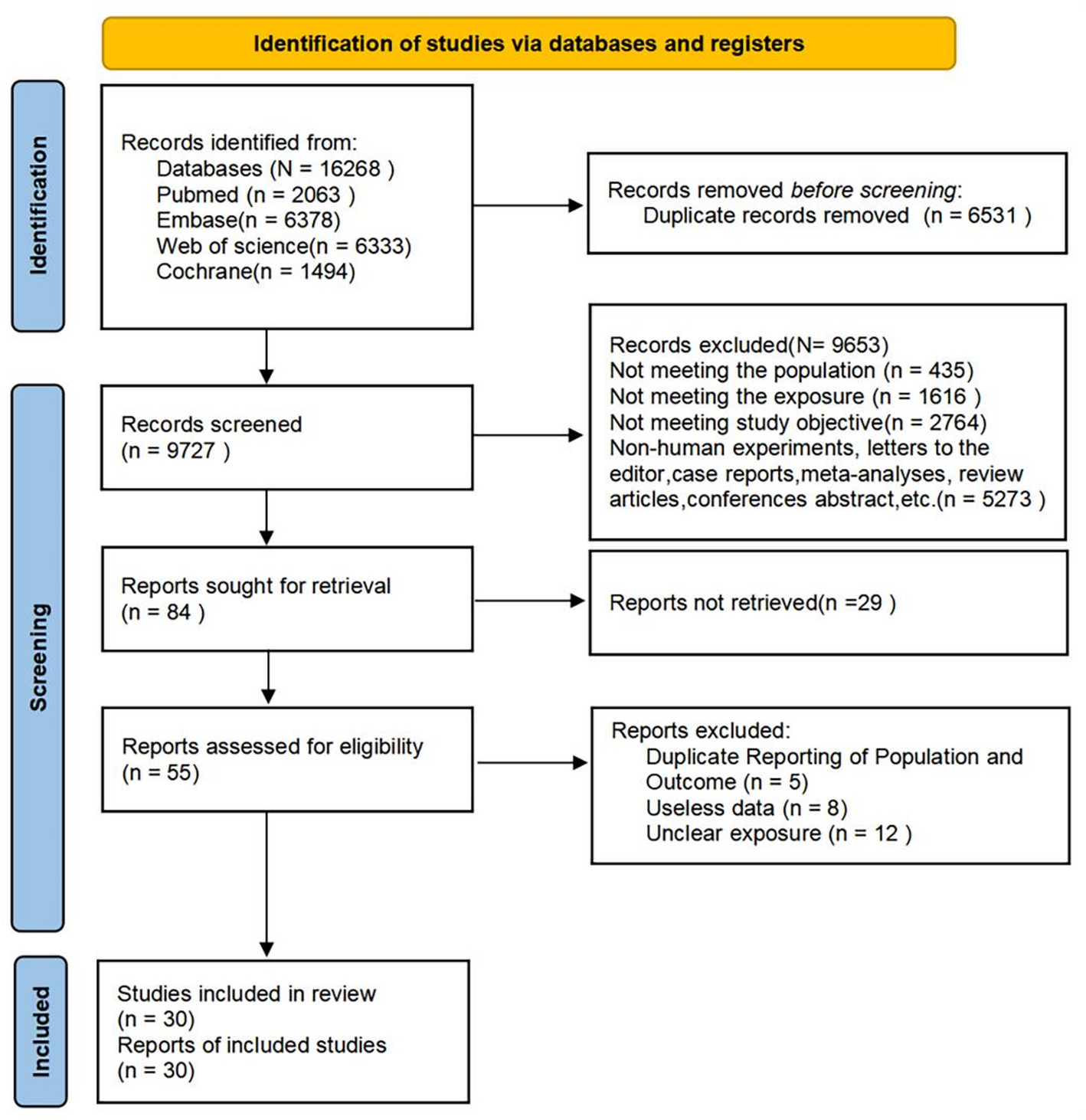


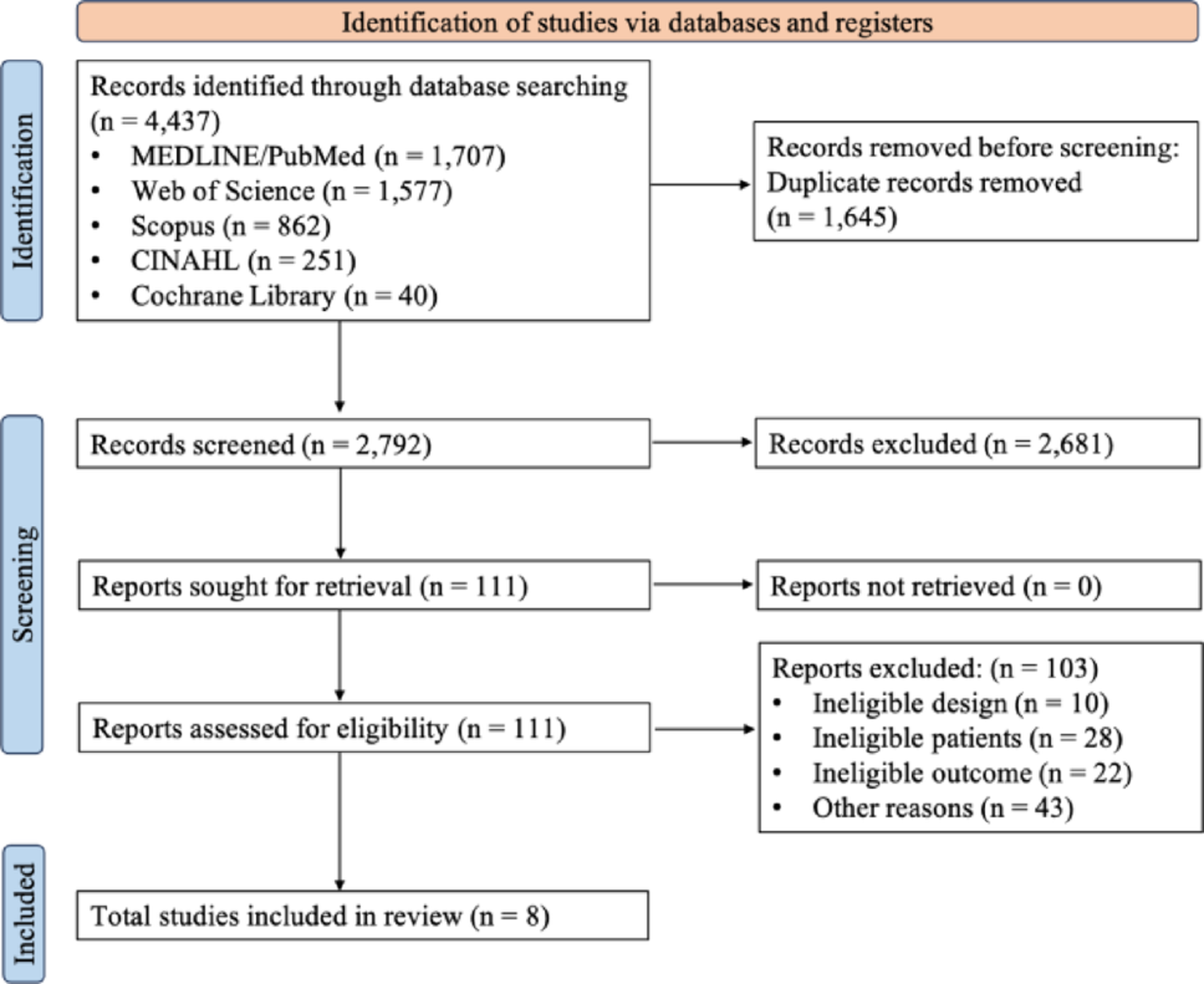
According to the process outlined in Fig. 1 above, we excluded patients lacking detailed pathological diagnosis, immunohistochemical results, and survival information, resulting in a total of 3197 patients being included in our study. The basic information of all patients is presented in Table 1. In summary, 41% of the patients in the study were aged between 51 and 65, 99.6% were female, 53.6% were unmarried, and 73.9% were white. Regarding pathological information, 100% of patients were diagnosed with de novo stage IV, 34.4% had T4 tumors, and 78.7% had lymph node metastasis. Concerning treatment, while 74.1% of patients received chemotherapy, the proportion of patients who underwent surgery was significantly lower, at only 32.1%. Regarding organ metastasis, bone remained the most common site for breast cancer patients with liver metastasis, affecting 56.6% of patients, followed by the lung at 32.7%. The percentages of patients testing positive for ER, PR, and HER-2 were 65.3%, 50.4%, and 40.9%, respectively. The mean OS and CSS for patients included in the study were 32.9 months and 35.1 months, respectively.
Table 1 Basic information for all patients included in this study3.2 Selection of variables in our nomogramWe conducted univariable and multivariable Cox regression analyses for all the variables listed in Table 1, determining their respective weights in OS and CSS. Initially, we performed a univariable analysis of the 16 variables, revealing that 14 of them displayed statistical significance. Subsequently, a multivariable analysis was conducted on these 14 variables to identify the final variables associated with OS and CSS, respectively (refer to Tables 2 and 3). The findings indicated that, with the exception of patient gender and whether radiotherapy was administered, all other variables demonstrated significant correlations with the OS and CSS of BCLM patients, thus warranting inclusion in the subsequent construction of the nomogram.
Table 2 Univariable and multivariable Cox regression analysis of OS in BCLM patientsTable 3 Univariable and multivariable Cox regression analysis of CSS in BCLM patients3.3 Nomogram construction and validationFollowing univariable and multivariable Cox regression analyses, we identified a total of 14 variables suitable for constructing the nomogram. These variables were found to significantly correlate with both OS and CSS. Among them are age, marital status, race, tumor grade, T stage, lymph node metastasis, surgery, chemotherapy, bone metastasis, lung metastasis, brain metastasis, ER status, PR status, and HER2 status. Utilizing these variables, we developed 1-year, 3-year, and 5-year nomograms for OS and CSS, respectively. These nomograms include individual scores and total scores, with the total score determined based on the individual scores computed using the nomogram. These scores enable the evaluation of patients’ 1-year, 3-year, and 5-year OS and CSS outcomes (refer to Figs. 2A and 3A).
Fig. 2
Nomogram and model assessment for predicting 1-, 3-, and 5-year overall survival (OS) in BCLM patients. A The OS nomogram for BCLM patients. B The calibration plots in the training cohort for 1-year, 3-year, and 5-year OS. AUC values of ROCs of the nomograms for 1-year, 3-year, and 5-year OS. C The ROC curves of training cohort. D The decision curve analyses (DCA) of the nomogram and other factors’ overall survival for the training cohort. E The calibration plots in the verification cohort for 1-year, 3-year, and 5-year OS. F The ROC curves of validation cohort. G The decision curve analyses (DCA) of the nomogram and other factors’ overall survival for the validation cohort. AUC Area under Curve, ROC Receiver Operating Characteristic
Fig. 3
Nomogram and model assessment for predicting 1-, 3-, and 5-year cancer-specific survival (CSS) in BCLM patients. A The CSS nomogram for BCLM patients. B The calibration plots in the training cohorts for 1-year, 3-year, and 5-year CSS. AUC values of ROCs of the nomograms for 1-year, 3-year, and 5-year CSS. C The ROC curves of training cohort. D The decision curve analyses (DCA) of the nomogram and other factors’ cancer-specific survival for the training cohort. E The calibration plots in the verification cohorts for 1-year, 3-year, and 5-year CSS. F The ROC curves of verification cohort. G The decision curve analyses (DCA) of the nomogram and other factors’ cancer-specific survival for the verification cohort. AUC Area under Curve, ROC Receiver Operating Characteristic
Following the construction of the nomogram, we assessed its accuracy using various methods, including the concordance index (C-index), calibration curves, time-dependent receiver operating characteristic [10] curves, and decision curve analysis (DCA). For OS, the C-index values were 0.709 (95% confidence interval (CI]) 0.693–0.725) in the training cohort and 0.726 (95% CI 0.705–0.747) in the verification cohort. For CSS, the C-index values were 0.710 (95% CI 0.693–0.728) in the training cohort and 0.721 (95% CI 0.697–0.745) in the verification cohort (refer to Table 4). The calibration curves of the nomogram (Figs. 2B, E, 3B, and E) demonstrate a high level of agreement between predicted and observed survival probabilities in both the training and verification cohorts for OS and CSS, respectively. Furthermore, the time-dependent area under the curve [11] values of OS and CSS predictions at 1, 3, and 5 years are all greater than 0.75 in both the training and verification cohorts (Figs. 2C, F, 3C, and F), indicating a favorable discriminatory ability of our developed nomogram.
Table 4 The C-indices for predictions of OS and CSSDCA curves are now widely utilized to compare nomograms with other clinically relevant factors. Figures 2D, G, 3D, and G depict DCA curves for OS and CSS of the nomogram and other clinical factors in BCLM patients. Our findings reveal that, in comparison with other clinical factors, the DCA curve of our designed nomogram exhibits significant superiority, suggesting its enhanced suitability for clinical use in aiding physicians to make informed decisions.
3.4 Risk stratification and their subgroup survival analysisWe aggregated the scores for each variable of BCLM patients to derive the total score and subsequently determined the cutoff value using X-tile software (version 3.6.1; Yale University, New Haven, CT, USA) (refer to Fig. 4A and C). Based on the X-tile software analysis results, we categorized the OS and CSS of BCLM patients into three risk levels: high-risk, medium-risk, and low-risk. Specifically, for OS, the high-risk, medium-risk, and low-risk groups for BCLM patients correspond to scores > 450, 305–460, and < 305, respectively (see Fig. 4B). Similarly, for CSS, the high-risk, medium-risk, and low-risk categories for BCLM patients are defined as scores > 437, 289–437, and < 289, respectively (refer to Fig. 4D).
Fig. 4
Risk stratification by X-tile software, the subgroup and their survival analysis. A The cut-off values of BCLM patients for OS. The black dot means the OS distinction point. B Risk stratification of OS in BCLM patients. The blue color is the low-risk group, the gray color is the medium-risk group, and the purple color is the high-risk group. C The cut-off values of BCLM patients for CSS. The black dot means the CSS distinction point. D Risk stratification of CSS in BCLM patients. The blue color is the low-risk group, the gray color is the medium-risk group, and the purple color is the high-risk group. E The Kaplan–Meier survival curves of three risk subgroups of BCLM patients for OS. F The Kaplan–Meier survival curves of three risk subgroups of BCLM patients for CSS
Utilizing this risk stratification, we generated Kaplan–Meier survival curves for BCLM patients across different risk levels. The 5-year OS rates were 35.0%, 11.3%, and 3.02% for high-risk, medium-risk, and low-risk BCLM patients, respectively (see Fig. 4E). Likewise, the 5-year CSS rates were 39.9%, 14.1%, and 1.6% for high-risk, medium-risk, and low-risk BCLM patients, respectively (refer to Fig. 4F). Notably, the differences among the three risk subgroups for both OS and CSS were statistically significant.
3.5 Web-based dynamic nomogram publicationWe have officially released our web-based nomograms for predicting OS in BCLM patients (Fig. 5A) and CSS (Fig. 5B). These nomograms are accessible at the following links: (https://osnomogram-xyhospital.shinyapps.io/BCLM-OSnomogram/) (accessed on 9 February 2024) and (https://cssnomogram-xyhospital.shinyapps.io/BCLM-CSSnomogram/) (accessed on 9 February 2024). You can utilize these platforms to perform data calculations and conduct risk analysis.
Fig. 5
The web-based dynamic nomogram. A Web-based dynamic nomogram of OS of BCLM patients (https://osnomogram-xyhospital.shinyapps.io/BCLM-OSnomogram/) (accessed on 9 February 2024). B Web-based dynamic nomogram of CSS of BCLM patients (https://cssnomogram-xyhospital.shinyapps.io/BCLM-CSSnomogram/) (accessed on 9 February 2024)
Comments (0)