
Remember me



We recruited patients from the Dementia Center, Shin-Kong Wu Ho‐Su Memorial Hospital, Taiwan, to participate in this study. Out of 45 potential candidates, 22 provided their informed consent and were subsequently enrolled in the study. Patients were included in the study if they met the following criteria: (1) were aged at least 65 years; (2) had been diagnosed with MCI according to Petersen’s criteria [4] ; (3) had received a global rating of 0.5 on the Clinical Dementia Rating (CDR) scale; and (4) could walk at least 10 m unaided. Patients were excluded if they had: (1) dementia; (2) a cerebral tumor; (3) a history of cerebral infarction or hemorrhage; (4) any other known neurodegenerative or neuropsychiatric condition; (5) any orthopedic disease that would make participation in the study difficult; or (6) fewer than six years of education (elementary school).
Study designWe conducted the study as a randomized controlled trial and ensured double-blinding (both raters and participants). Participants were randomly assigned to either the tDCS + ICCT group or the sham + ICCT group using numbers placed in sealed envelopes. Training was administered three times a week for five weeks, totaling 15 sessions. Each session lasted for 40 min of Switch training. The tDCS group received stimulation during the initial 20 min of each session, while the sham group underwent stimulation for 30 s at the start of the session. The participants were trained individually by an experienced research assistant. Each participant also underwent baseline assessments one day before the intervention and post assessments one day after the intervention, all conducted by a rater who was unaware of the group assignments. The rater performed two independent tests: a cognitive assessment followed by a gait assessment. The study protocol was approved by the ethics committee of Shin-Kong Wu Ho‐Su Memorial Hospital (IRB number: 20200709D, August 28, 2020). Additionally, this experiment is registered as a clinical trial at http://www.clinicaltrials.in.th/ (TCTR 20,220,328,009).
tDCSFor the stimulation, we utilized a battery-operated constant DC Stimulator Plus (NeuroConn, Ilmenau, Germany). The stimulation delivered consisted of 2 mA of current via a pair of sponge electrodes soaked in a saline solution. These electrodes measured 50 × 70 mm (3,500 mm²) in size and were positioned to deliver optimal stimulation to the left DLPFC. Specifically, we placed the anode centrally over the F3 position according to the international 10–20 system, and the cathode was positioned at Fp4, corresponding to the contralateral right supraorbital region, as illustrated in Fig. 1. In the tDCS + ICCT group, this direct current was administered continuously for 20 min, following a 10-second ramp-up period. The duration of 20 min is considered both safe and commonly used in clinical research [26, 27]. The stimulation parameters and electrode montage for the sham + ICCT group were identical to those in the tDCS + ICCT group, with the exception that the current was only delivered for 30 s and then gradually reduced to 0 mA. This approach aimed to replicate the tingling sensation associated with active stimulation, making it indistinguishable from anodal tDCS treatment, although we assume it had negligible effects on the participants’ brains. We monitored the impedance of the electrodes throughout the entire stimulation period in all sessions to ensure that it remained below 5 kΩ for safety.
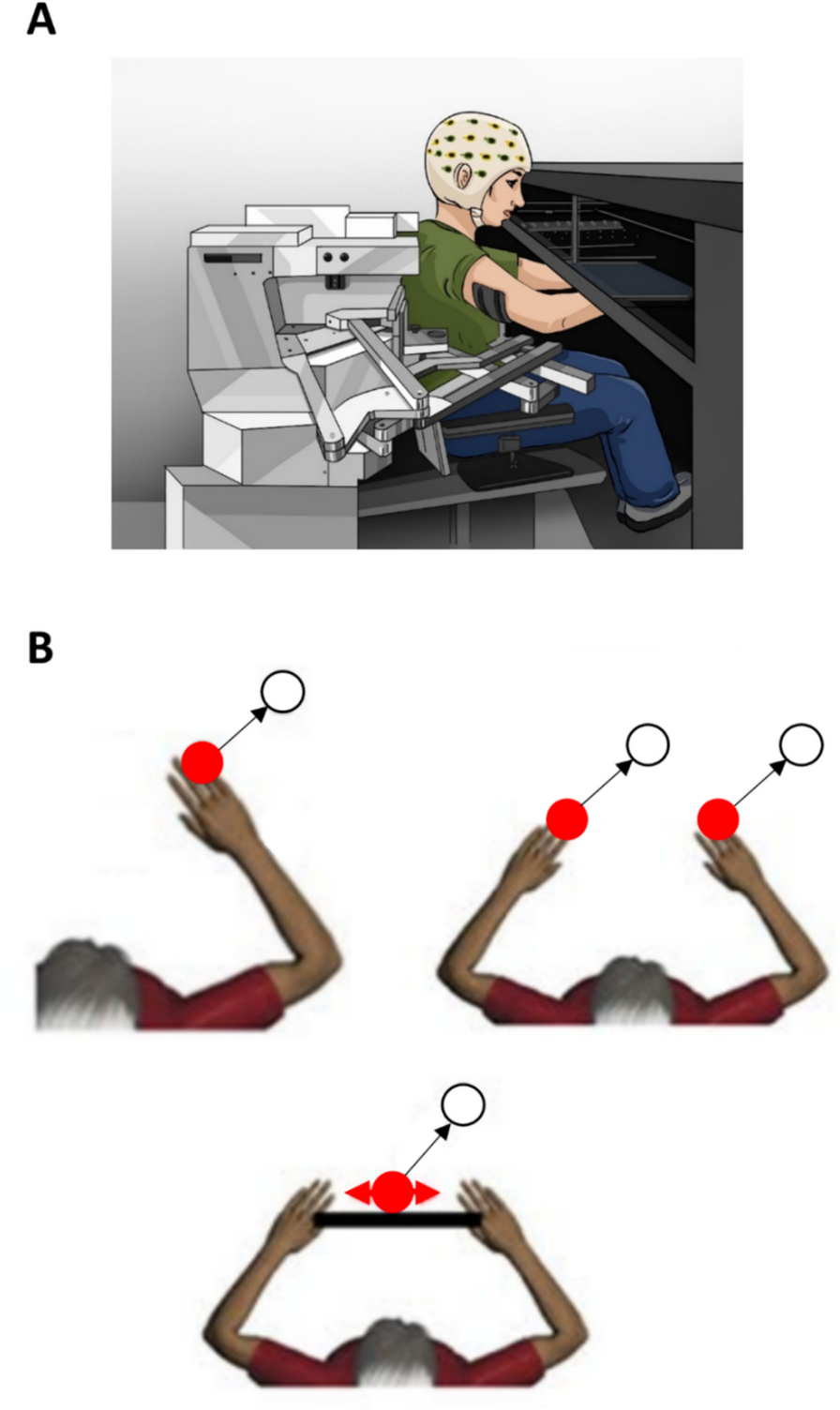
Fig. 1
Left: example of a subject receiving the tDCS + ICCT protocol. Right: the tDCS montage
ICCT programThe ICCT program covered executive function, attention, and memory domain and was administered via a commercial virtual-reality game console developed by Nintendo Switch in 2017. Nintendo Switch games can be played either on the console’s own screen or on a linked television screen. The participants used Switch Joy-Cons, which have infrared motion sensors on both sides, to detect their hand movements. We selected the following interactive games from the game library to use for cognitive training. During each session, all seven games we selected were played. Participants consistently began at the foundational level, with the program automatically adjusting difficulty based on their performance throughout the 40-minute duration.
1.Finger Calculation: A picture on the screen showed a number of fingers held up on two hands. The participants had to calculate the sum and mimic the number with their own fingers in front of the Joy-Con camera as quickly as possible.
2.Finger Gymnastics: The screen displayed a series of rock-paper-scissors graphics. The participants had to imitate the displayed graphics in front of the camera as quickly as possible.
3.Rock, Paper, Scissors Test: A picture of a hand in the rock, paper, or scissors position appeared randomly on the screen. The participants had to respond with the appropriate gesture to win the round according to the standard rock, paper, scissors rules.
4.Bird and Box Counting: The participants had to calculate the number of birds or boxes illustrated on the screen and select the correct number with the Joy-Con.
5.Working Memory: Groups of pictures appeared randomly on the screen. The participants had to select the picture that had appeared in the previous group from three pictures on the next screen. To increase the difficulty level, the participants had to select the photo that had appeared two rounds previously.
6.Five in a Row: On a grid on which pieces can be placed at the intersections of horizontal and vertical lines, the participant had to try to make a horizontal, vertical, or diagonal line of exactly five pieces before the computer did so.
7.Card Memory Test: Twenty playing cards were displayed face-down on the screen. The participant and the computer took turns turning over single cards and then replacing them face-down again. The participant had to try and memorize these. The one whose turn it was had to try and find another card that matched the one turned over (based on their memory of previously revealed cards). If they found one, they would take both cards. The game finished when all the face-down cards had been turned over and taken.
Outcome measuresCognitive performance1. Global cognitive function
We assessed the participants’ global cognitive function using the Montreal Cognitive Assessment (MoCA). In the MoCA, the total score ranges from 0 to 30, with a higher score indicating better global cognitive function [28].
2. Working memory
We evaluated participants’ working memory using the N-back task. In this test, the participants had to indicate whether the current position matched the one used one step previously (1-back) and two steps previously (2-back) in the sequence. We tallied the number of trials the participant answered correctly [29]. The participants also completed the visual working memory (VWM) test. In this test, three colored squares were randomly displayed for 100 ms on a screen. After a retention interval of 900 ms, another set of colored squares was displayed. The participant was asked to indicate whether the current display was identical in color to the previous one. We calculated the reaction time as d-prime (d’) [30].
3. Episodic memory
We assessed the participants’ episodic memory using the Chinese Version of the Verbal Learning Test (CVVLT). Nine nouns were recited and the participants had to attempt to recall them immediately and again after a delay of 15 min. The number they recalled correctly was recorded, and this process was repeated four times [31].
4. Executive function
We assessed the participants’ attention, task-switching ability, and executive function using the Trail Making Test (TMT) parts A and B. In TMT-A, the participant had to connect 25 numbers in the correct sequence, and in TMT-B, they had to link 12 numbers with the 12 signs of the zodiac in the correct order as quickly as possible [32]. We recorded the time the participant took to complete each test. We also assessed their executive function using the Tower of London (ToL) task. The participant had to move colored beads arranged on three vertical rods to achieve a particular goal arrangement. Successive tasks increased in complexity and the participant had to perform two to five moves to reach the goal in each case. We analyzed the total time they took and their accuracy [33].
Gait performanceWe measured the participants’ gait parameters using the Gait Up system (Gait Up, Lausanne, Switzerland). The system consists of a wearable device, and the measurement instrument has good validity and reliability [34]. GaitUp utilizes two wireless inertial sensors equipped with triaxial accelerometers, along with one tablet. The sampling frequency of the Gait Up system is 128 Hz. These sensors are secured using two rubber clips, attached to the dorsal side of the participants’ shoes, just below the lateral malleolus. The sensors can establish a wireless connection with a tablet for data control. In each trial, upon pressing “start” on the tablet, a three-second countdown is displayed before the “go” signal, during which the sensors undergo automatic calibration. The walking path was a straight corridor with 10 m marked as the starting and finishing points for each trial. The system automatically excludes the first and last gait cycles (acceleration and deceleration) and then computes the average gait parameters during the 10 m. A PDF report is instantly generated and uploaded to the cloud after participants complete each trial. We set up two tasks to assess the participant’s gait performance: (1) a single task, involving walking at the participant’s preferred speed; (2) a dual task, involving walking while conducting a subtraction task, in which the participant had to start from a randomized three-digit number and subtract three from it serially (e.g., 100, 97, 94 …). We asked the participant to perform three trials of each task and recorded the following spatiotemporal parameters: speed (m/s), stride length (m), and cadence (step/min). We took the average of each parameter from the measurements made during the three trials. We quantified dual-task interference based on the DTC of speed, calculated as: DTC of speed (%) = [single-task walking speed – dual-task walking speed) / single-task walking speed] x 100% [35]. Finally, we defined gait variability as the coefficient of variation of stride length (i.e., standard deviation/mean × 100%).
Data analysisWe analyzed the sociodemographic, neuropsychological, and gait data using SPSS 20.0 (SPSS, Chicago, IL, USA). Descriptive statistics were generated for all variables, and distributions were expressed as means ± standard deviations or as counts. Initially, we assessed the uniformity of data distribution. Next, between-group differences in baseline characteristics were examined using independent t-tests or chi-squared tests. To evaluate the effects of ICCT on participants’ cognitive function, we conducted a two-way repeated-measures analysis of variance (ANOVA). The model included two groups, the timepoint of assessment (before or after the intervention), and the interaction between group and timepoint. Post-hoc analyses were performed with Bonferroni correction. Statistical significance was defined as p < 0.05. Partial eta-squared (η2) was calculated and used to indicate the effect size.
Comments (0)