Surgery-induced necrotizing scleritis (SINS) can be triggered by any type of ocular surgical intervention, and the latency period is highly variable, ranging from first postoperative day to years after surgery [1]. Women are more affected, and the average age is fifth decade of life [1]. Pterygium excision is the most associated ocular surgery and autoimmune diseases are specially related in the cataract extraction cases [1, 2].
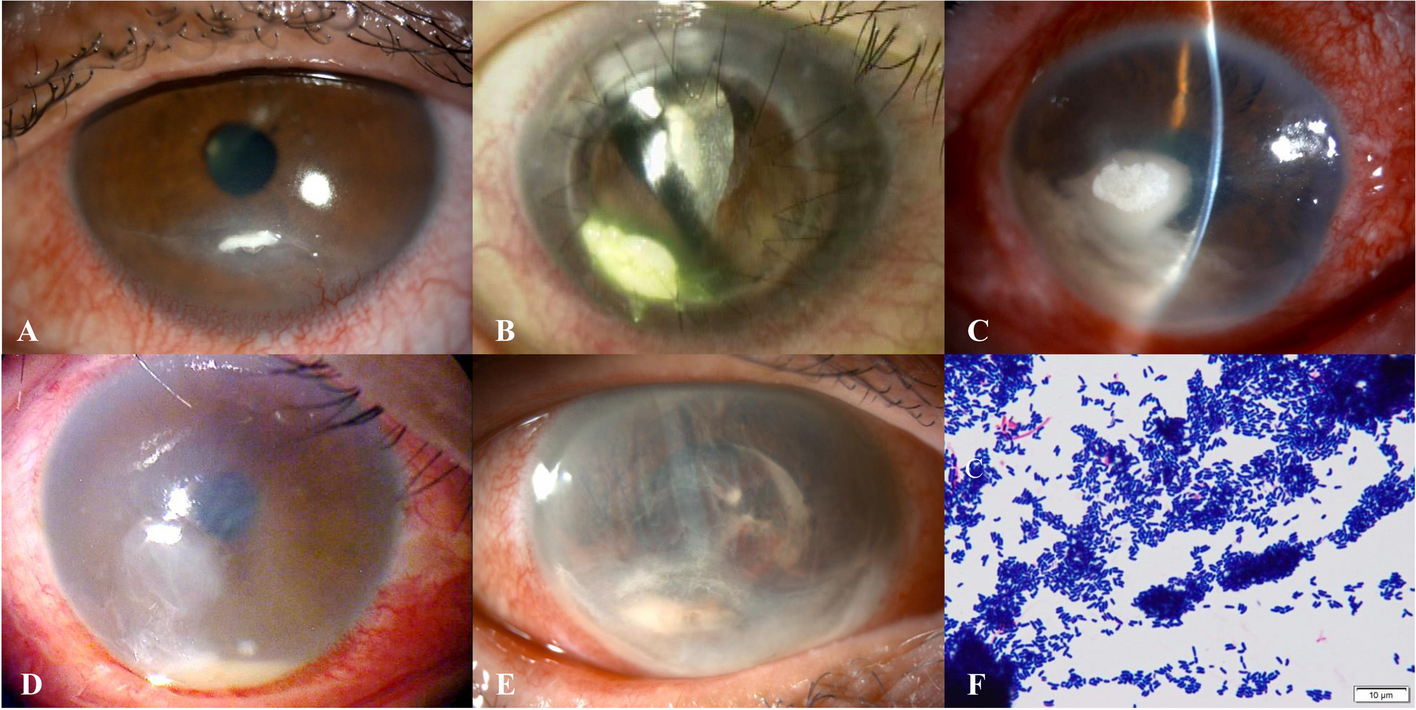
Predicting SINS poses a considerable challenge, as postoperative scleral thinning can go unnoticed, leading to a delayed diagnosis. In the early stages of the condition, patients may encounter symptoms like conjunctival redness and mild discomfort, which are frequently misinterpreted as dry eye disease or conjunctivitis, prolonging the diagnosis and treatment process [1]. In advanced cases, patients typically manifest significant pain, visual impairment, peripheral corneal ulcers, scleral necrosis, and the development of anterior staphylomas [1].
This entity involves a common induction mechanism (ocular surgery) and a characteristic pathological finding (scleral necrosis) [1]. Physical trauma caused by excessive cauterization or cryotherapy, chemically induced damage with antimetabolites, compression-related ischemia, like tighten sutures, as well as autoimmune local activation, represent a wide range of pathogenic mechanisms that can induce scleral necrosis [1, 2, 5]. Diabetes is also related due to the pro-ischemic inflammatory environment that exerts [6]. All these induce a slowdown in surgical wound healing, that can lead to a secondary infection [7]. The overlap between these mechanisms complicates the diagnosis and its corresponding treatment.
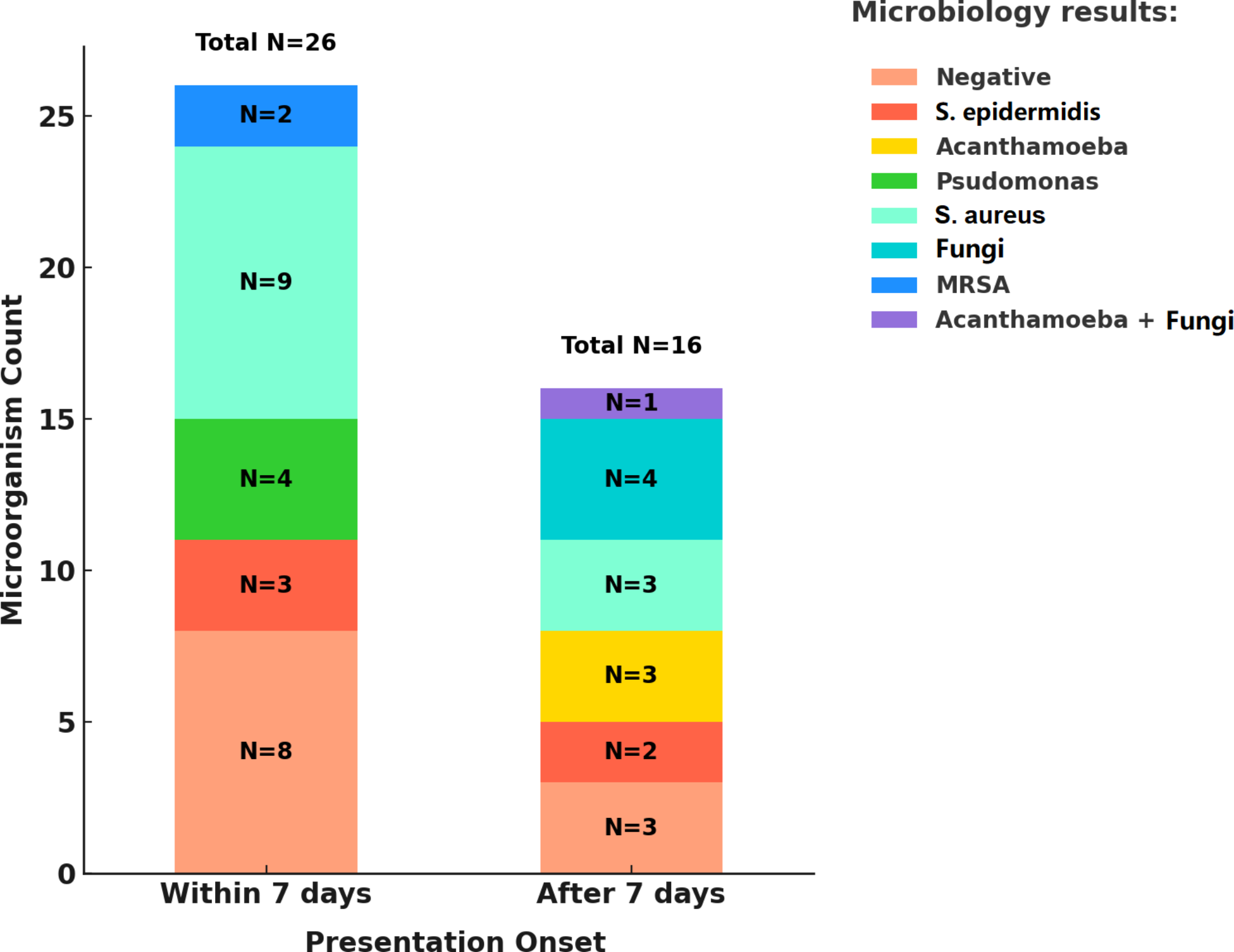
Considering the multiple aetiologies related to necrotizing scleritis, a comprehensive study should be conducted to discard primary infectious scleritis or underlying autoimmune involvement [5]. The research should include complete blood count, erythrocyte sedimentation rate, C-reactive protein, liver and kidney function tests, serum complement levels, antinuclear antibody, rheumatoid factor, antineutrophil cytoplasmic antibody, anti-citrullinated protein antibody, and serum angiotensin-converting enzyme levels [5]. To rule out infectious involvement, wound scrape for microbiological culture, or for scleral biopsy, and intraocular samples for PCR are necessary [2, 5, 7]. In addition, testing for tuberculosis, syphilis, HIV infection, hepatitis B and C, herpes simplex and varicella-zoster viruses should be performed [2, 7].
Due to the devastating consequences for the eye, early detection and treatment are fundamental. Topical antibiotics and/or antifungals are often empirically administered [1, 2]. The presence of mucopurulent discharge or hypopyon increases suspicion of an infectious aetiology, thus initiating topical and systemic antibiotic treatment is recommended [7]. Topical corticosteroids are associated with poor wound healing [1, 8]. Therefore, they have the potential to perpetuate the scleral thinning process, as it happens in the early stages of our case. As adjunctive treatment, oral doxycycline (100 mg/day) can also be added for its anticolagenolytic effect [8].
Systemic nonsteroidal anti-inflammatory drugs are useful at diagnosis [1, 5]. However, long-term use is not recommended due to their side effects [8]. Oral prednisone is considered first-line therapy in non-infectious necrotizing scleritis, with an initial immunosuppressive dose of 1 mg/kg/day gradually tapered based on clinical recovery [1, 5, 8]. Due to the stage 3a CKD of our patient, the corticosteroid doses were inferior to usual. Intravenous methylprednisolone for 3 days has shown efficacy in patients with severe inflammation, as it happens in our case [1, 8]. A patient with SINS will require a combination with nonsteroidal immunomodulatory therapy to enhance efficacy and avoid the long-term adverse effects of corticosteroids [1, 5, 8]. Some medications used include methotrexate, azathioprine, mycophenolate mofetil, cyclophosphamide cyclosporine and tacrolimus [5, 8, 9]. We choose the first one due to his safety profile in elderly and comorbidly patients [8].
A better understanding of the immunopathogenesis of ocular inflammatory diseases, as well as the development of new molecules, has enriched our therapeutic arsenal and created more effective treatment approaches [10, 11]. Monoclonal antibodies against TNF-α (all except Etanercept), IL-1 inhibitors (Anakinra), IL-6 inhibitors (Tocilizumab), and anti-CD20 (Rituximab) targeted-drugs have been shown to control inflammation and reduce scleritis flares, allowing for a corticosteroid-sparing effect [5, 8, 10, 11]. TNF-α inhibitors like Adalimumab or Infliximab are used as first-line biological agents [12, 13]. Adalimumab is the only biologic treatment approved for non-infectious uveitis and it has been used in other case reports with excellent clinical outcomes [13].
However, patients with active and progressive scleral necrosis will require immediate conjunctival debridement [14]. Apart from obtaining a scrape when infection is suspected, conjunctival resection results in a decrease of protease concentration, including collagenase, and a temporary interruption of the local inflammatory process [1, 14]. The use of cyanoacrylate glue after surgical debridement can help prevent neutrophil migration [1]. Conjunctival and Tenon’s flap grafts, as well as amniotic membrane transplantation, can also be used [1]. However, when uveal tissue is exposed, a tectonic procedure with scleral patch graft is preferred [1, 5, 15].








Comments (0)