Limited and conflicting data have been reported so far on the clinical utility of CYP2C19 genotyping in stroke/TIA patients of non-East Asian ancestries. The fact that 12 out of 15 studies included in the previous meta-analysis of Pan et al. [16] were conducted on East Asian patients, primarily of Han-Chinese ancestry, can be explained, among other reasons, by a higher frequency of CYP2C19 LOF alleles in this population in comparison to other ethnic groups, with intermediate and poor metabolizers accounting for about 59% of East Asians compared to 29% of white Europeans and 23% of Americans [12]. In addition, the incidence of stroke is higher in China than in USA and Europe [30, 31], with first-ever strokes per year in China accounting for almost a quarter of the global incident cases of stroke [32]. However, given population growth and ageing, the global lifetime risk of stroke in Western countries is expected to rise in the next few decades, with forecasts suggesting that the number of stroke patients will increase in Europe by 27% within 2047 [31] and that strokes events will double in the USA by 2050 [33]. Thus, given the recent publication of additional studies, in the present study we conducted an up-to-date meta-analysis to obtain a more precise estimation of the association between CYP2C19 LOF allele status and the clinical response to clopidogrel in non-East Asian patients with stroke or TIA.
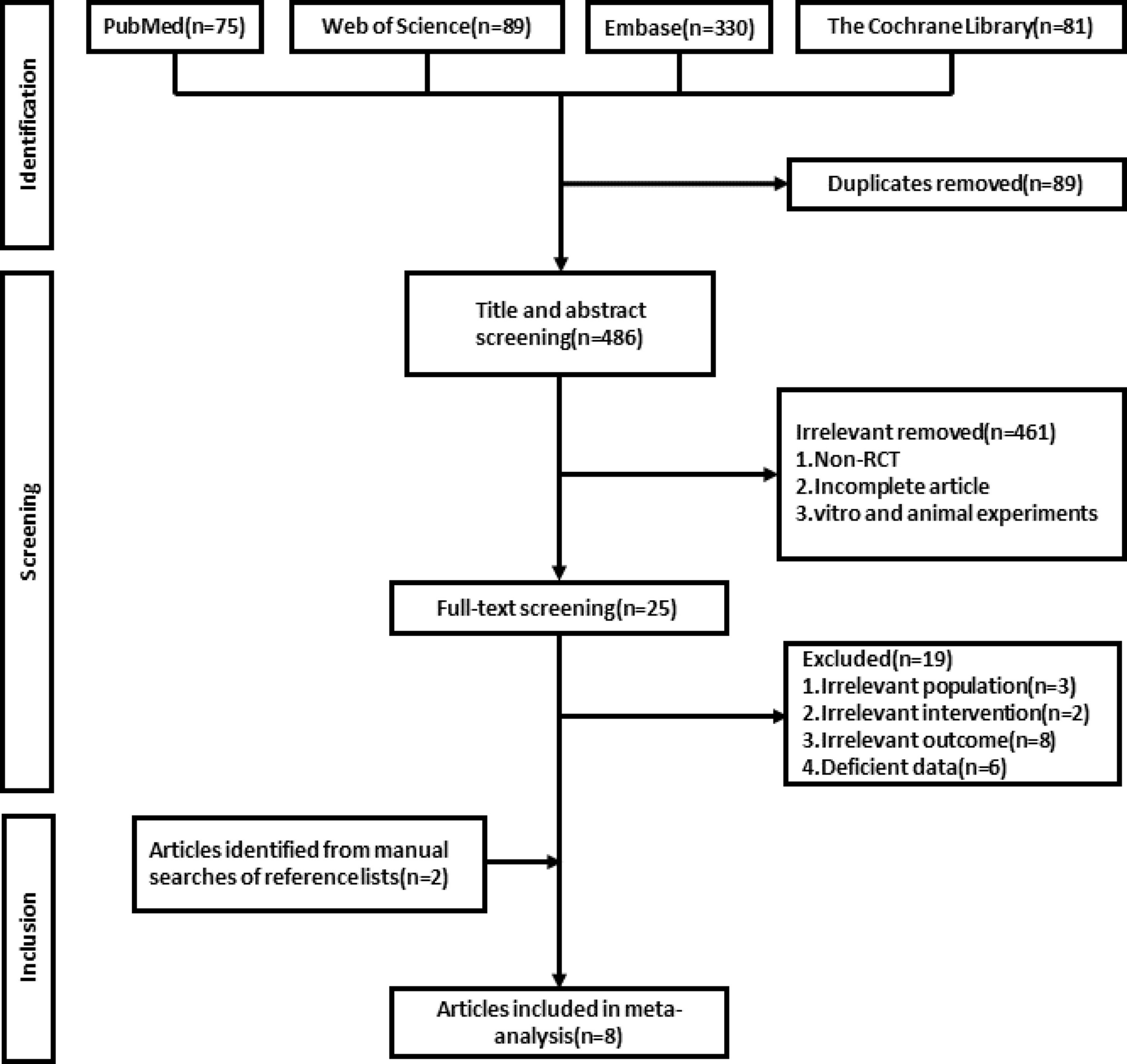
The present updated meta-analysis comprises 8 studies with a total number of 1673 clopidogrel-treated stroke/TIA patients, that is more than twice as many non-East Asian patients compared with the previous meta-analysis of Pan et al. [16]. The pooled results showed that carriers of CYP2C19 LOF alleles are at significant higher risk of stroke after receiving clopidogrel-based antiplatelet therapy, compared to non-carriers (RR: 1.68, 95%CI: 1.04–2.71, P = 0.03), and this association was scored as “moderate quality” using the GRADEpro tool. In contrast, no difference was found in the risk of composite vascular events (RR: 1.15, 95%CI: 0.58–2.28) or bleeding (RR: 0.84, 95%CI: 0.38–1.86), despite a “very low quality” evidence was identified for these two outcomes. Similarly to the overall analysis, a significant association of CYP2C19 LOF alleles status was found with stroke in the subgroup of patients with European ancestry.
Overall, our findings provide moderate evidence that carriers of CYP2C19 LOF alleles derive less benefit from clopidogrel treatment after ischemic stroke or TIA, suggesting that CYP2C19 genetic testing may be considered to personalize antiplatelet therapy in non-East Asian patients. In such populations, if aspirin is contraindicated, clopidogrel dose escalation or antiplatelet agents not influenced by CYP2C19 genetic variants, such as ticagrelor and ticlopidine, could be alternative P2Y12 inhibitors for CYP2C19 LOF alleles carriers after ischemic stroke or TIA. It is noteworthy that our pooled estimates, which stem form data of non-East Asian studies, are in line with those obtained in the East Asian subgroup of stroke/TIA patients from the previous meta-analysis of Pan et al. [16], which found that East-Asian carriers of CYP2C19 LOF alleles are at higher risk of stroke in comparison with non-carriers (RR: 1.93, 95%CI 1.55–2.39, P < 0.00001), while no difference emerged among patients of East Asia in the risk of bleeding (RR: 0.92, 95%CI: 0.58–1.45, P = 0.72). Overall, these results suggest a similar impact of CYP2C19 LOF alleles on the efficacy and safety of clopidogrel in stroke/TIA patients of East-Asian ancestry compared to those of non-East Asian origin. Therefore, our findings further corroborate current CPIC and DPWG guidelines for CYP2C19 genotype-guided clopidogrel therapy in stroke/ TIA patients [12, 34], which provide evidence of a moderate strength recommendation of alternative antiplatelet agents for CYP2C19 LOF allele carriers and do not suggest specific recommendations according to patient’s ethnicity, although based primarily on evidence available in Asian patients.
We acknowledge several limitations of our study that should be taken into account for the correct interpretation of the results. Firstly, the present systematic review consists of a limited number of studies with a relatively low sample size. Despite our attempt to conduct a comprehensive pooled analysis of all available published reports, some publications were not eligible for the systematic review because of unavailability of corresponding authors to provide the data requested for the effect size calculation. Therefore, great caution is needed in the interpretation of our pooled risk estimates, a consideration which is also suggested by the results of leave-one-out meta-analyses showing lack of robustness of pooled estimates. Secondly, according to the inclusion criteria of the present systematic review, we considered only non-East Asian studies enrolling patients with stroke or TIA undergoing clopidogrel-based antiplatelet therapy. However, very few patients of East Asian ancestry could have been recruited in some of the included studies, as shown in Supplementary Table 2. Nevertheless, a significant association was still found in the subgroup of patients with European ancestry between carriers of CYP2C19 LOF alleles and higher risk of stroke, after clopidogrel-based antiplatelet therapy. Thirdly, the studies of the present systematic review differ with respect to some characteristics such as clopidogrel-based regimen, follow-up duration and CYP2C19 variant alleles analysed, which may have an impact on the effect size estimation. Nevertheless, little or no heterogeneity was observed in the pooled results, as shown by the I2 statistics. Fourthly, in almost all the included studies, investigation of loss-of-function CYP2C19 alleles was limited to CYP2C19*2 and CYP2C19*3 alleles, which represent the most frequent CYP2C19 LOF alleles among all populations. Other CYP2C19 alleles such as CYP2C19*9 and CYP2C19*10, which are known to determine a reduced enzymatic activity [12], have been overlooked by the authors of the studies included in the present systematic review. However, the risk that this could have affected our findings is rather low, given the very low frequency of CYP2C19*9 and CYP2C19*10 alleles among the different populations [12]. Moreover, our pooled estimates are not adjusted by factors known to have an impact on metabolic activation of clopidogrel via CYP2C19. For instance, the co-administration of CYP2C19 inhibitors, such as proton pump inhibitors (PPIs) or some antidepressant drugs, reduces the efficacy of clopidogrel on platelets and may thus worsen the clinical outcome [35], while cigarette smoking is known to enhance clopidogrel-induced platelet inhibition, which may explain the higher relative benefit of clopidogrel among smokers [36, 37]. To address the latter limitation, a meta-analysis of individual participant data should be performed to obtain adjusted RRs and to assess the impact of factors, such as PPIs or antidepressants coadministration as well as cigarette smoking, on the association of CYP2C19 genotype with efficacy and safety of clopidogrel therapy in stroke/TIA patients. On the other hand, clinical risk factors and the CYP2C19 genotype can be integrated by the ABCD-GENE score to estimate the efficacy of clopidogrel-aspirin therapy [38]. The ABCD-GENE score, which incorporates age, BMI, chronic kidney disease, diabetes mellitus and CYP2C19 loss-of-function alleles, has been demonstrated among Chinese minor stroke/TIA patients to identify subjects at increased risk of stroke recurrence following clopidogrel-aspirin therapy [39]. Future investigation is thus required to assess validity of the ABCD-GENE score tool in stroke/TIA patients of other ethnic origins, including Europeans. Furthermore, it is well known that CYP2C19*2 and *3 alleles are associated to a decreased antiplatelet activity, as demonstrated by ex vivo platelet reactivity testing in on-treatment patients [15, 40, 41]. However, platelet reactivity analysis was conducted by only one of the included studies [27], which results were consistent with a strong association of platelet activity with CYP2C19*2 allele status. Lastly, only two studies [27, 29] included in our analysis have reported the ischemic stroke subtypes according to TOAST classification and, in both these studies, cases with undetermined cause were a large proportion (40% and 53.7%, respectively). This could have impacted the strength of the association between CYP2C19 LOF allele status and efficacy of clopidogrel therapy in preventing stroke recurrence, given that in a proportion of these patients antiplatelet therapy might not have been the best secondary prevention strategy. In fact, among other causes, occult non-valvular atrial fibrillation (AF) could have been the culprit of some cases of stroke recurrence, which therefore should not be considered linked to the lack of clopidogrel efficacy in LOF allele carriers. Moreover, concomitant presence of known and properly treated AF in those rare patients requiring also an antiplatelet therapy for several reasons could be potential source of stroke recurrence, given the possibility of anticoagulation failure or lack of patients’ compliance. Unfortunately, only [28] and [29] have reported the number of patients with known AF, which were a small number (Supplementary Table 2). Nevertheless, the pharmacogenetic analysis of the ACTIVE trial [42] has shown a lack of difference between CYP2C19 genotypes and outcomes in AF patients.
In conclusion, the present systematic review provides updated pooled risk estimates for the association of CYP2C19 LOF allele status with efficacy and safety of clopidogrel-based antiplatelet therapy in non-East Asian patients with stroke or TIA, including Europeans. The results of pooled analyses from non-East Asian studies support that carriers of CYP2C19 LOF alleles have a significant increased risk of stroke following TIA or ischemic stroke when treated with clopidogrel. These results provide some evidence of potential clinical utility of CYP2C19 genotyping to personalize antiplatelet therapy in non-East Asian patients with stroke/TIA, including those of European ancestry. However, due to the limited sample size of this systematic review, further large and possibly multicentric studies enrolling stroke/TIA patients of European and other non-East Asian ancestry are warranted. Such studies are strongly needed not only to confirm our findings but also to investigate gene–gene and gene–environment interactions, along with the adjustment of confounding factors, for the association of CYP2C19 genotype with efficacy and safety of clopidogrel in patients with stroke or TIA.

Comments (0)