VTE is one of the most common complications after KA. Our meta-analysis found that age over 30 years, BMI over 25, and D-dimer over 0.62 mg/L are significant risk factors for VTE following KA. Limited evidence also suggests an association between oral contraceptive use and a higher risk of VTE following KA.
The meta-analysis revealed that patients undergoing KA who are over 30 years old had a 1.59-fold higher risk of postoperative venous thrombosis compared to those under 30. Hashimoto et al. [15] identified age as a risk factor for venous thrombosis following KA. Previous studies have reported that the cumulative incidence of VTE increases with advancing age [21]. Firstly, progressive degenerative changes in the vascular system occur with aging, characterized by the formation of atherosclerotic plaques. These pathological processes lead to vascular wall thickening, reduced elastic fibers, luminal narrowing, and decreased vascular compliance. Such structural alterations disrupt hemodynamics by elevating local shear stress and blood viscosity, significantly increasing blood stasis. This promotes platelet activation and fibrin deposition, ultimately driving pathological thrombus formation [22]. Secondly, aging is associated with abnormal blood rheological parameters, including significant age-dependent increases in whole blood viscosity and plasma viscosity. Concurrently, upregulated expression of platelet activation markers on platelet membranes enhances their propensity for aggregation and occlusion [23]. Aging is accompanied by heightened activity of key intrinsic coagulation factors (e.g., Factors VIII and IX), while anticoagulant mechanisms such as antithrombin III (AT-III) activity and the protein C system exhibit functional decline [24, 25]. Finally, advancing age is often correlated with decreased physical activity and functional decline in vascular systems, further elevating thrombotic risk [26, 27]. Although biological mechanisms and most studies indicate that VTE risk increases with age, there was significant heterogeneity in the critical age thresholds among our included literature. Madeleine et al. [17] used 50 years as the critical threshold, while Wu et al. [10] employed 32 years. This inconsistency in threshold values likely contributed to the observed publication bias. Given that there are currently no standardized guidelines for establishing these critical values, and based on current research that commonly uses 30 years as the age threshold [7, 28], we recommend that patients over 30 years of age undergoing KA should be closely monitored for the risk of VTE.
The meta-analysis revealed that patients undergoing KA with BMI over 25 had a 1.23-fold higher risk of postoperative VTE compared to those under 25. Previously, Kanaya et al. [8] considered a BMI over 25 to be a risk factor for VTE. Zhong et al. [7] also pointed out that a BMI over 25 is a risk factor for VTE. Firstly, patients with a BMI over 25 often have lipid metabolism disorders, such as increased triglycerides and decreased high-density lipoprotein (HDL) levels, while HDL has an antithrombotic effect [29, 30]. Secondly, those with a BMI over 25 frequently exhibit increased platelet activity and elevated levels of plasminogen activator inhibitor-1 (PAI-1), leading to decreased fibrinolytic function, making the blood more prone to clotting. Inflammation from adipose tissue is believed to contribute to increased thrombosis [31]. Finally, patients with a BMI over 25 often have an abnormal accumulation of visceral fat, particularly characteristic changes associated with abdominal obesity, which can lead to impaired venous return from the lower limbs due to mechanical compression. Additionally, the reduced exercise tolerance associated with obesity significantly decreases daily activity levels, resulting in decreased skeletal muscle pump efficiency, thereby increasing the risk of thrombosis [32, 33].
This meta-analysis demonstrated that a postoperative D-dimer over 0.62 mg/L served as an independent predictive factor for VTE following KA. While Wu et al. [10] identified elevated postoperative D-dimer levels as a significant risk determinant for VTE with 86.5% sensitivity at the 0.62 mg/L threshold, Sugimoto et al. [9] failed to establish D-dimer elevation as a significant thromboembolic risk indicator. D-dimer, a specific byproduct of fibrinolytic system activation, quantitatively reflects the degradation of cross-linked fibrin. Its elevated levels were validated as a predictive biomarker for venous thrombus formation in multiple clinical validations [34]. Despite variations in D-dimer cutoff values across relevant literature, it is noteworthy that multiple studies have confirmed that elevated D-dimer levels are significantly associated with the occurrence, progression, and severity of VTE [35,36,37]. Therefore, patients with D-dimer >0.62 mg/L should be closely monitored for VTE formation.
The meta-analysis found an association between oral contraceptive use and a higher risk of VTE following KA. Meaidi et al. [38]and Traven et al. [18] also found that oral contraceptives are a risk factor for VTE following KA. Current evidence indicates that oral contraceptives can promote a hypercoagulable state by activating genetic susceptibility in carriers of the Factor V Leiden mutation and by increasing the activity of procoagulant proteins such as prothrombin (Factor II), thereby raising the risk of VTE [38, 39]. In addition, combined oral contraceptive pill (COCP) use increases VTE risk in the general population by elevating plasma fibrinogen activity and enhancing platelet aggregation [40, 41]. Although our meta-analysis results are supported by extensive literature, the limited sample size inevitably introduces bias into our findings. Nevertheless, we must remain attentive to the risk of VTE in patients taking oral contraceptives who undergo knee surgery. Given the limited amount of evidence, it is currently difficult to draw definitive conclusions regarding oral contraceptives as a risk factor for VTE following KA. Future studies with standardized exposure definitions, adequate control of key confounding factors, and complete perioperative management information are needed to verify this association and provide higher quality evidence for clinical practice.
Our meta-analysis found no evidence that surgical duration, diabetes, smoking, gender, or hypertension are risk factors for VTE after KA. Regarding the influence of diabetes, research conclusions are divergent. Hu et al. [42] identified it as a risk factor, while Joo et al. [16] reached conclusions consistent with ours, finding no significant correlation between diabetes and postoperative VTE risk. Notably, although diabetic patients face increased risk of vascular diseases due to chronic hyperglycemia and various pathophysiological changes, aggressive pharmacological intervention can effectively improve vascular outcomes, and some anti-hyperglycemic treatment regimens may modulate VTE risk [43]. Concerning gender factors, Linnemann et al. [44] suggested that female sex might be a risk factor for VTE after KA, which differs from our findings. A possible explanation is that hormone replacement therapy and pregnancy may indeed increase postoperative VTE risk [45, 46], but it should be noted that elective surgical interventions are typically not recommended during pregnancy. Regarding hypertension, our findings align with those of Nazarzadeh et al. [47], neither confirming a correlation between hypertension and increased post-operative VTE risk. Furthermore, our analysis failed to establish significant correlations between surgical duration or smoking and VTE risk following KA. The interpretation of these results should consider the minimal differences in cutoff values across studies, the lack of standardized criteria, and the interference of various subjective factors that may affect outcome assessment.
Recent work on enhanced visualization techniques and advancements in anterior cruciate ligament repair during KA have shown how refined arthroscopic procedures can achieve faster mobilization and shorter surgical duration, both of which can impact the risk of VTE [48, 49]. Regarding the prevention of VTE after KA, different guidelines provide varying recommendations. The current guidelines published by the American College of Chest Physicians and the American Academy of Orthopaedic Surgeons suggest that routine thromboembolic prophylaxis is not recommended for patients without a known history of VTE, while patients with a history of thrombosis may receive prophylaxis [50]. In contrast, European guidelines advocate for pharmacological prophylaxis for KA even in patients who are not at high risk for VTE [51]. Currently, there is still controversy in the medical field regarding the routine provision of thromboembolic prevention after KA. The use of medications for thrombus prevention may increase the heterogeneity of outcome measures. Additionally, existing literature often excludes patients with a history or predisposition to thrombosis, and different studies employ various mechanisms to reduce risk bias. Therefore, the results of meta-analyses remain of significant reference value for the prevention of VTE after KA. Furthermore, in recent years the application of artificial intelligence (AI) and machine learning (ML) models in predicting postoperative thromboembolism in orthopedics has improved the accuracy of VTE detection and prediction [52, 53]. This makes it particularly important to understand the risk factors for postoperative VTE after KA in order to identify, predict, and prevent VTE in high‑risk patients.
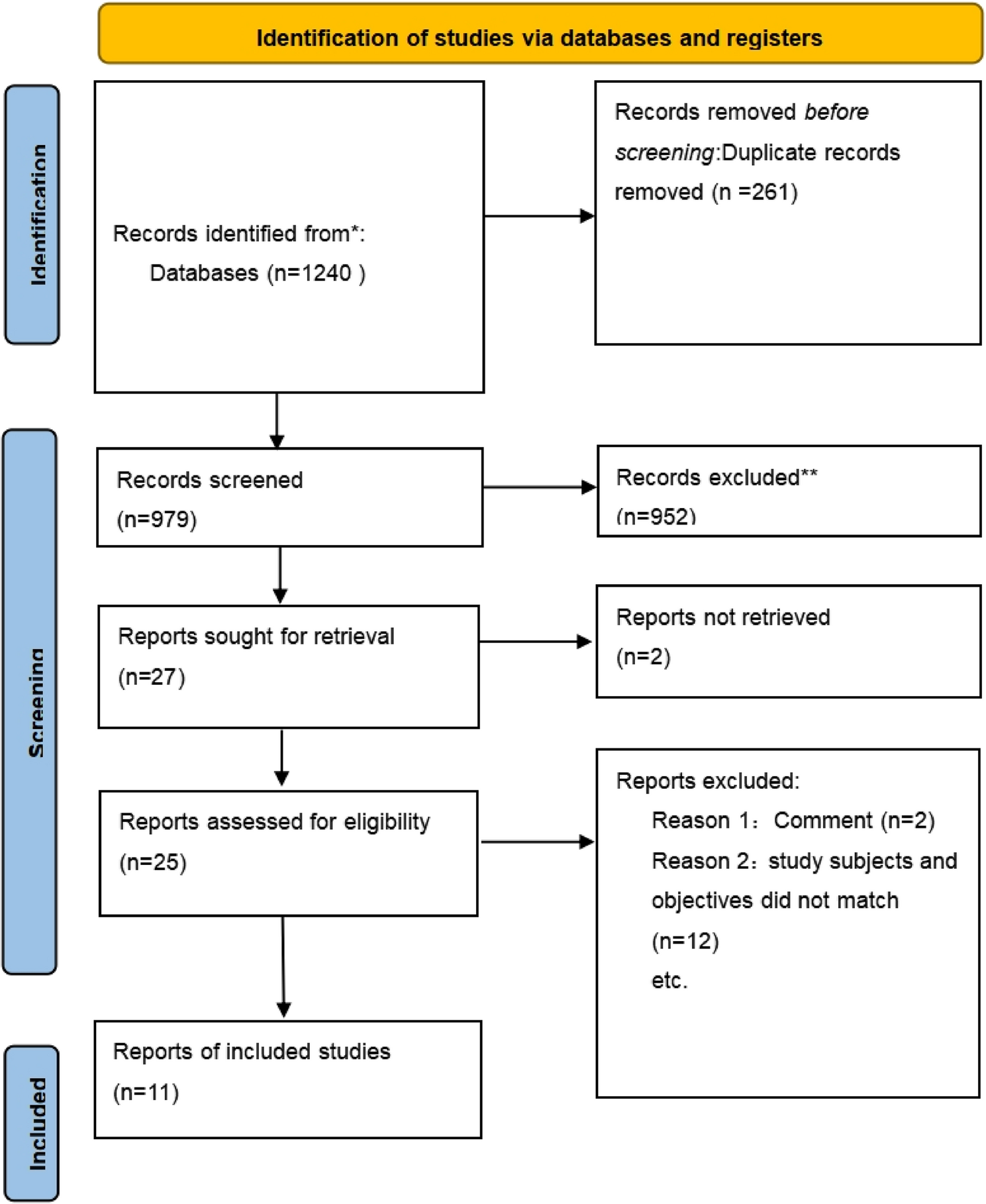
This study is a comprehensive analysis of risk factors for VTE following KA. A thorough search across four databases and manual searches ensured the complete inclusion of relevant studies. However, this research still has several limitations. Firstly, many studies only provided data from univariate analyses rather than multivariate analyses, meaning the results might be influenced by confounding factors. Secondly, differences in surgical types across studies, the choice of cutoff values for independent risk factors, variations in surgical techniques among different surgeons, and the impact of surgical duration on the diagnosis of VTE may contribute to increased heterogeneity. Finally, the inclusion of five case-control studies in this analysis could also contribute to higher heterogeneity, and compared to cohort studies, case-control designs have weaker causal inference capabilities.


Comments (0)