This PMS study reaffirms the safety and effectiveness of evolocumab and adds to the established body of evidence by providing real-world evidence of high-risk patients with ASCVD or FH in Korea, among whom no safety concerns, such as hemorrhagic events, were observed with evolocumab. Importantly, our findings indicate that achieving very low LDL-C levels (< 20 mg/dL) at week 12 did not result in an increased occurrence of AEs, which is consistent with the FOURIER OLE [8] and prior Japanese PMS study [23]. Notably, in our study, median baseline LDL-C was 100.2 mg/dL, despite use of high-intensity statin and ezetimibe in half of all patients and high-intensity statin in a quarter. Nevertheless, following 3 months of evolocumab treatment, median LDL-C was reduced by 70.6% and was maintained at < 30 mg/dL until week 52. Evolocumab on-treatment effectively maintained low LDL-C levels, while off-treatment LDL-C levels increased, regardless of the type of baseline ASCVD (MI, angina, or ischemic stroke [cerebral infarction]).
Our study demonstrated lower AE rates with evolocumab compared to major randomized, controlled trials (RCTs), primarily due to shorter follow-up periods and differences in AE monitoring between RCT and PMS settings. Despite these variations, the safety profile of evolocumab in high-risk Korean patients indicated that it was well tolerated in this PMS study, aligning with findings from RCTs [10, 11, 24]. In our study, the AE rate up to 56 weeks of evolocumab treatment was 23.9%, with the most frequent AEs being headache (2%), chest pain, and myalgia (1.5% each), and no SAEs were ADRs. The rate of ADRs was 2.4%, including a low rate of myalgia (0.9%) and headache (0.4%), while asthenia, fatigue, injection-site redness, nausea, ocular discomfort, and abnormal white blood cell count were reported in 0.2% of patients. In FOURIER, the AE rate did not differ between evolocumab and placebo (77.4%), and in a subanalysis of 2723 Asian patients compared with other patients (n = 24,841), no significant between-group differences in the incidence of AEs, including hemorrhagic stroke, rhabdomyolysis, new-onset diabetes, or cognitive decline, were shown [25]. In other subanalyses of FOURIER, no increased risk of muscle-related events, cataract, new-onset diabetes [26, 27], neurocognitive events [7, 28], or hemorrhagic stroke [11, 29] were shown, even with up to more than 8 years of evolocumab treatment [7].
Prior real-world data also reported a favorable safety profile of evolocumab in populations across Europe [17, 18], North America [19, 20], and in prior Korean studies [21, 22]. Prior Korean studies reported no significant differences in safety outcomes between evolocumab and non-evolocumab treatment in patients with recent acute MI (AMI), including myalgia and fatigue [22]. Another observational study (ZERBINI) of 578 patients with ASCVD and/or FH who initiated evolocumab at sites across Canada, Mexico, Columbia, Kuwait, and Saudi Arabia reported AE rates of 3.3%, with the most common AEs being balance disorder/dizziness (0.9%), myalgia (0.5%), and headache (0.5%); no SAEs were reported [20]. Thus, despite theoretical concerns regarding PCSK9 inhibitors and safety, particularly with low LDL-C levels achieved, previous study results, our PMS study results, and those of FOURIER-OLE, support an overall favorable safety profile of evolocumab in patients with very low LDL-C (< 20 mg/dL).
In clinical trials in patients with elevated LDL-C despite LLT, including in patients with at least one CV risk factor [10] or with ASCVD (MI, non-hemorrhagic stroke, PAD) in FOURIER [11], evolocumab significantly reduced LDL-C, by about 60%. Overall, in this study, a third of the patients with ASCVD had diabetes and, in FOURIER, it was shown that reductions in LDL-C with evolocumab were similar regardless of the presence of high-risk comorbid conditions such as diabetes [26]. This was also seen in our study; median LDL-C was reduced from baseline to week 12 by 70.6% in the overall effectiveness analysis set and by 68.0% in the subgroup with diabetes. In FOURIER-OLE, LDL-C reductions observed early post-evolocumab initiation were maintained long term, during up to 8.6 years of follow-up [6, 7]. In the analysis of FOURIER that compared evolocumab treatment between Asian and other patients (baseline LDL-C 89 mg/dL and 92 mg/dL, respectively), at 48 weeks, mean percentage (66% vs 58%) and absolute (61 mg/dL vs 55 mg/dL) LDL-C reductions were greater in Asian patients [25].
The LDL-C lowering effect of evolocumab was observed regardless of the baseline LLT regimen, which, despite guideline recommendations for the use of ezetimibe in high-risk patients with ASCVD receiving maximally tolerated statin therapy [14, 15], included high-intensity statin plus ezetimibe in just over half of all patients (51.9%), statin only in a third (33.2%), and ezetimibe only in 1.3%. This is a reflection of real-life clinical practice where adherence to guidelines/treatment may be suboptimal, yet additional LDL-C lowering for CV risk reduction in high-risk patients WITH ASCVD is paramount to reduce the burden of further CV events [9]. Additionally, patients who were on-treatment with evolocumab at specific time points (week 12, 24, or 52) maintained their LDL-C levels. However, with the caveat of the limited interpretation due to the small sample size, patients on off-treatment (≤ 20 patients) at these time points experienced an increase in LDL-C levels, with the week-52 data appearing similar to the week-12 data. This underscores the importance of continuing evolocumab treatment for sustained LDL-C reduction. In a previous study of Korean AMI patients who underwent PCI, those who received a single-dose injection of evolocumab during PCI, along with statin/ezetimibe, had a greater LDL-C reduction (78.4% vs. 45.6%) and a higher rate of achieving LDL-C < 55 mg/dL (97.7% vs. 60.0%) within 1–3 weeks compared to those without evolocumab [21]. Importantly, evolocumab has shown consistent LDL-C lowering in various populations, including those at increased risk of further CV events. In the observational real-world HEYMANS (cHaractEristics of hYperlipidaeMic pAtieNts at the initiation of evolocumab and treatment patternS) European registry of 1951 patients with hypercholesterolemia (many not on LLT) initiating evolocumab in routine clinical practice [30, 31], and in patients with ASCVD or FH across North and South America, the Middle East and Western Asia (ZERBINI) [20], baseline LDL-C was 153.9 mg/dL and 131.5 mg/dL, respectively; with evolocumab treatment, median reduction from baseline was 58.0% and 70.2%, respectively, which remained stable over follow-up.
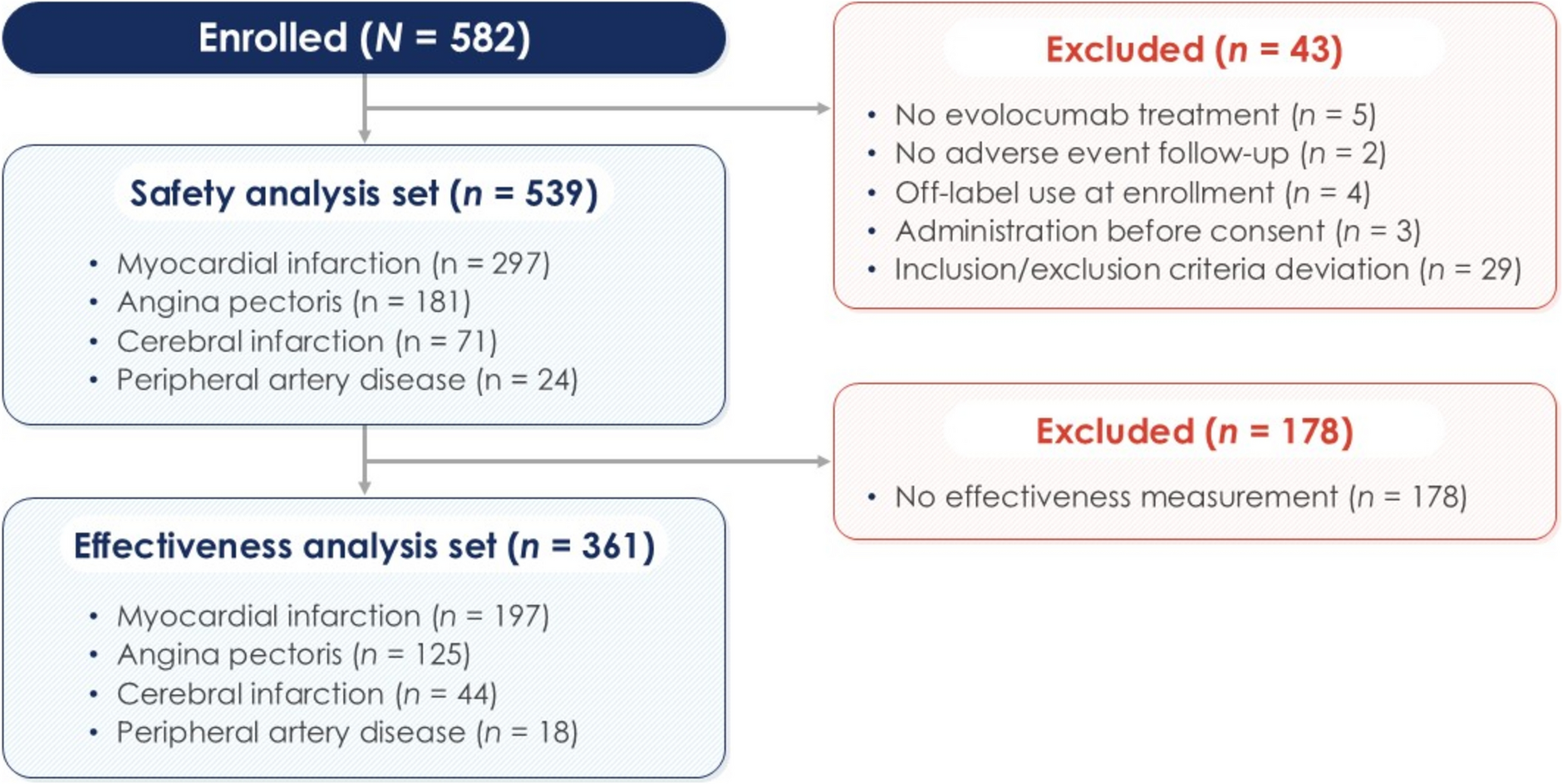
This multicenter PMS study provides evidence by including a considerable number of evolocumab-treated patients from 43 centers (539 patients for safety evaluation and 361 patients for effectiveness evaluation), with up to three follow-up LDL-C assessments during up to 56 weeks of follow-up, and fills a gap in the real-world clinical evidence of evolocumab in Asian populations. Nevertheless, there are several limitations of this study. First, the absence of a control group in this study limits the ability to determine comparative safety or effectiveness and whether the observed effects of evolocumab are due to the treatment itself or other external factors. Second, the clinical information for evolocumab-treated patients was collected by physicians using CRFs; hence, there are limitations to the collected information regarding AEs and effectiveness, particularly as LDL-C was measured as part of routine clinical practice and not as part of the study procedure. Lastly, the population with FH in our study does not appear to include patients with HoFH, although 1.3% were of unknown type.
In conclusion, evolocumab demonstrated a favorable safety profile and effectively reduced LDL-C levels in Korean patients with ASCVD or FH. There were no cases of hemorrhagic stroke following evolocumab treatment, and achieving very low LDL-C levels (< 20 mg/dL) at week 12 was not associated with increased incidence of AEs. Additionally, evolocumab led to a 70.6% median LDL-C reduction at 12 weeks, with levels sustained below 30 mg/dL through week 52 in on-treatment patients, regardless of ASCVD subtype. These findings support the use of evolocumab as a valuable therapeutic option.


Comments (0)